

Clinician's Compass | Physio Needs a Sister Act
The irrefutable case for the inevitable independent Australian Physiotherapy College
At some point in the last few years, you’ve probably heard it.
“We can fit you in with our Nurse Practitioner if you like.”
And if you said yes, you got a highly competent clinician who knew their field, sorted your problem, and sent you on your way. No fuss. Exactly what healthcare is supposed to look like.

What you probably didn’t know — what most physios don’t know either — is that elite healthcare professional sitting across from you was the product of 34 years of deliberate structural work.
A spark in 1990. A decade of pilots. A breakaway college in 2003. A 14-year fight to remove a funding constraint that should never have existed.
Access to Medicare Benefits Scheme (MBS) and Pharmaceutical Benefits Scheme (PBS) items that only began in 2024.
That clinician didn’t happen by accident.
Physio could be that clinician. We aren’t. This is why.
The thing I took a decade to notice
It wasn’t a single moment that hit me in the head. It was a cluster.
I was stuck in the ‘here & now’ but increasingly I was looking at the ‘where am I going’, which is basically everyone once they’ve remained engaged in their profession for over a decade. Especially if despite increasing skill, expertise and training producing significant outcomes to both their customer (the patient) and the system (healthcare burden), they’ve seen no significant income increase over that time and there’s suggestions of none to come.
My patients needed me to have more autonomy, direct referrals to orthopaedic surgeons, access to Medicare rebates on MRI sets. They were sick of going back to their GP just to bother them for admin.
“Surely the physio career pathway of Titling and Specialisation unlocks these things?
Surely it’s more than words on a business card and a gold email signature?”
But I was wondering: what is the return on investment spending another $40–50,000 on another Masters degree — when I’m already quite active in my own professional development without it - spending thousands/year and hundreds of hours on continued learning.
Physios I respected, mentors — people who’d been in the profession long enough to have seen several reform cycles come and go — told me early on: “don’t bother with titling, they’re just words”. They then went on to say they’ve been hearing the same promises from the APA for decades.
I filed that away as professional cynicism. The kind of thing experienced, tired, veteran workers say to the new bright eyed and bushy tailed mature-aged kid.

So in March 2023, I emailed the APA as an APA member with three specific questions about titling.
Were there plans for external recognition for Titling and Specialisation?
Is there imminent access to Medicare on the horizon for Titled and Specialist Physios?
Was the experiential pathway for Musculoskeletal Titling even coming back?
The APA member support manager was polite. He reached out to different teams. He said the Head of the College of Physiotherapists would personally respond — titling fell within her remit.
She didn’t respond.
So I followed up.
I got ‘crickets’.
I left the APA nine months later. And nothing bad came of it.
I’ve been thinking about that silence ever since. Not as a grievance — I’m over it — but as data. Because that non-reply wasn’t negligence. It was a symptom of something structural. Something the APA cannot fix by trying harder, communicating better, or hiring a new head of college.
It took me over a decade to notice the massive conflict of interest. And I’m in the trade.

Having become despondent with the metaphorical poor state of my metaphorical clinical backyard I looked over the metaphorical clinical fence, to see what my metaphorical clinical neighbours were doing, and I found out what our metaphorical Sisters accomplished:
The Nurses had achieved something remarkable.
The Sister Act
The story goes…..
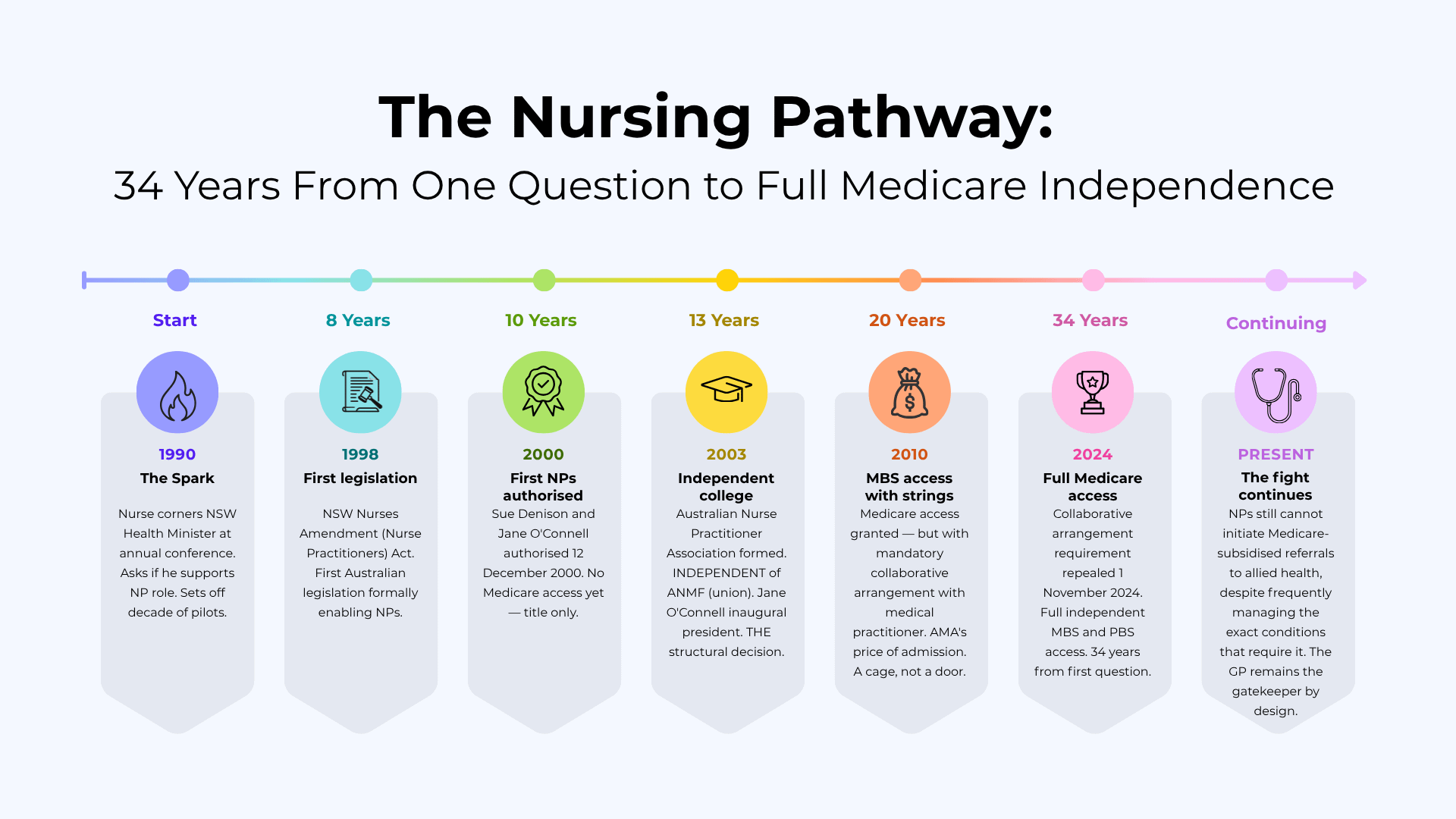
In 1990, a nurse at the NSW Nurses Association annual conference cornered the health minister and asked whether he supported the nurse practitioner role.

That question launched a decade of state-based pilots, legislative work, and evidence-building that was deliberate, methodical, and specifically designed to answer the objections before they were raised.
The pilots ran from 1992 to 1995 — ten of them, across rural and remote NSW. The settings were chosen deliberately, not the easy ones, but the communities where the workforce gap was so obvious that even the opposition couldn’t deny the need.


For my American readers, the kind of places where tumbleweed crosses the road more often than its townsfolk.
For my UK readers, Wales.
Places with no doctor, waiting months for a GP appointment that would never come. The evidence they generated wasn’t academic. It was political ammunition, carefully stockpiled for the arguments that were coming.
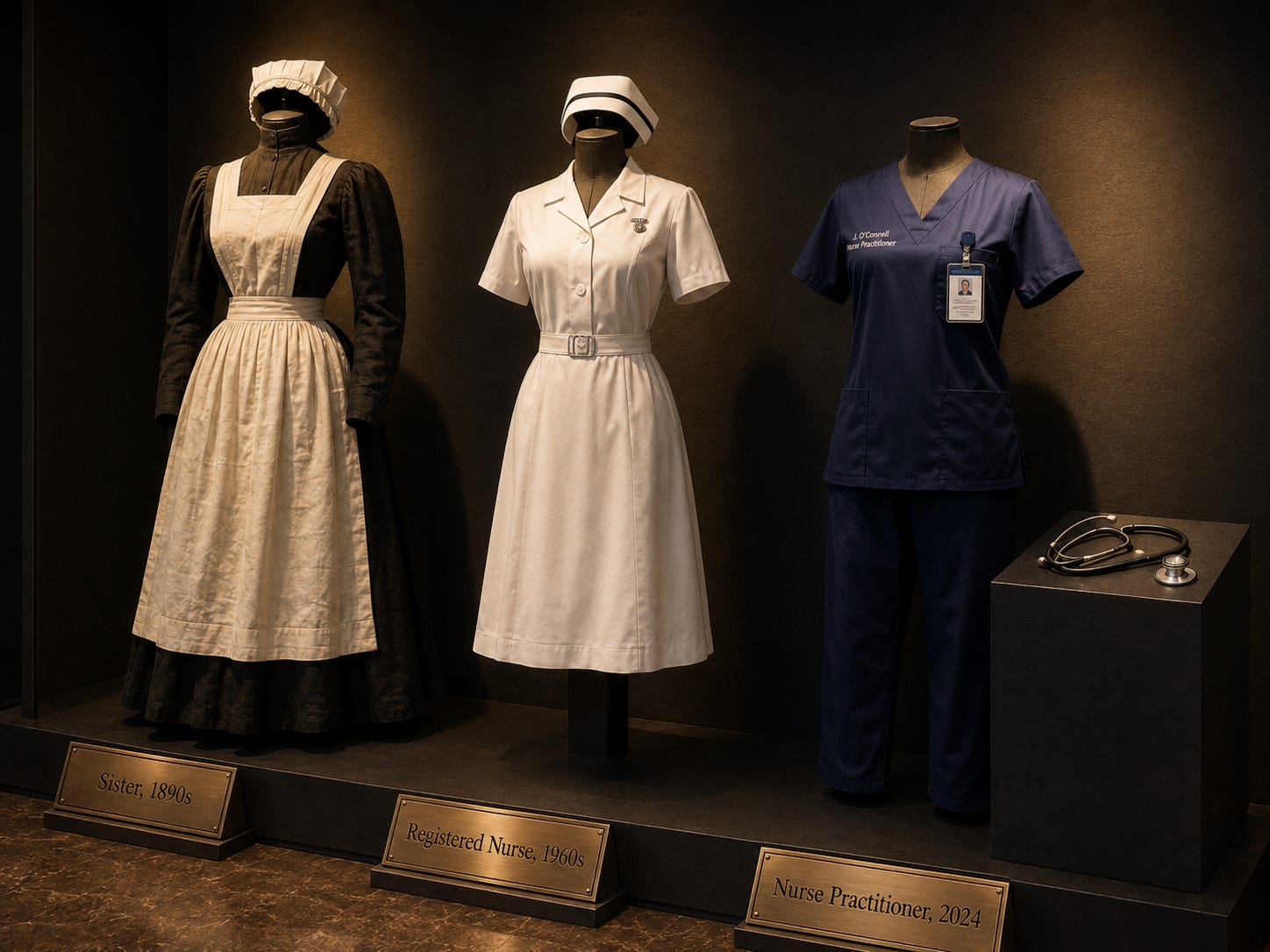
By 2000, Australia’s first two nurse practitioners were formally authorised — Sue Denison in rural Nundle, Jane O’Connell in emergency medicine in Sydney. The title existed. Medicare didn’t follow. For a decade they were legally nurse practitioners carrying the same funding access as a registered nurse, which is to say: the structure wasn’t built yet, and without the structure, the title was just a name.
By 2003, a group of them made the structural decision that changed everything. They formed an independent credentialing college — the Australian Nurse Practitioner Association, now the Australian College of Nurse Practitioners (ACNP) — completely separate from their union, the Australian Nursing and Midwifery Federation (ANMF). [1][2]

It was the most difficult part and the most necessary. The ANMF didn’t disappear — it kept fighting for wages, conditions, and ratios, which is exactly what unions are supposed to do.
But the NPs understood something that physio still hasn’t acted on: a union arguing for its own members’ expanded scope will always look like a pay claim. An independent college making the same argument looks like evidence. Same words, completely different weight, depending entirely on who’s standing behind them.
Three separate lanes:
The ANMF (union) fights for collective wages. Solidarity.
The ACNP (college) credentials advanced practice and advocates for it externally. Exclusivity.
The Nursing and Midwifery Board of Australia (NMBA) (regulator) handles registration. Regulation.
Each body credible in its domain because it only does one thing, and because doing only one thing means it has no conflicting incentive when it speaks.
None of it went smoothly.
The Australian Medical Association (union) called NP practice “third-world medicine.”

The Royal Australian College of General Practitioners (RACGP) (college) did the “they’re taking our jobs ” thing and then the “they’ll be a risk to continuity of care” thing and generally pushed back against any Medicare item that might allow a patient to see an NP without first passing through a GP.
These weren’t fringe positions.
They were institutionalised through funding rules, governance frameworks, and Medicare eligibility requirements that took decades to unpick — and some of which haven’t been unpicked yet.
As of 2026, NPs still cannot initiate Medicare-subsidised referrals to allied health, including physiotherapy, despite frequently managing the exact conditions that require it. The GP remains the gatekeeper by design, not by clinical necessity, and both the AMA and RACGP have consistently defended that design.

The people who fought hardest against newly endorsed NPs were sometimes not doctors at all — they were senior nurses, protective of territory they’d spent careers building, threatened by colleagues who were suddenly authorised to do more.

The collaborative arrangement requirement — mandatory medical supervision as the price of Medicare access — was a cage the NPs accepted in 2010 as the political price of getting through the door, then spent the next fourteen years trying to dismantle.
The MBS Review Taskforce rejected all fourteen NP recommendations for expanded Medicare access. Not some of them. Every single one, in a committee heavily weighted toward medical representation.
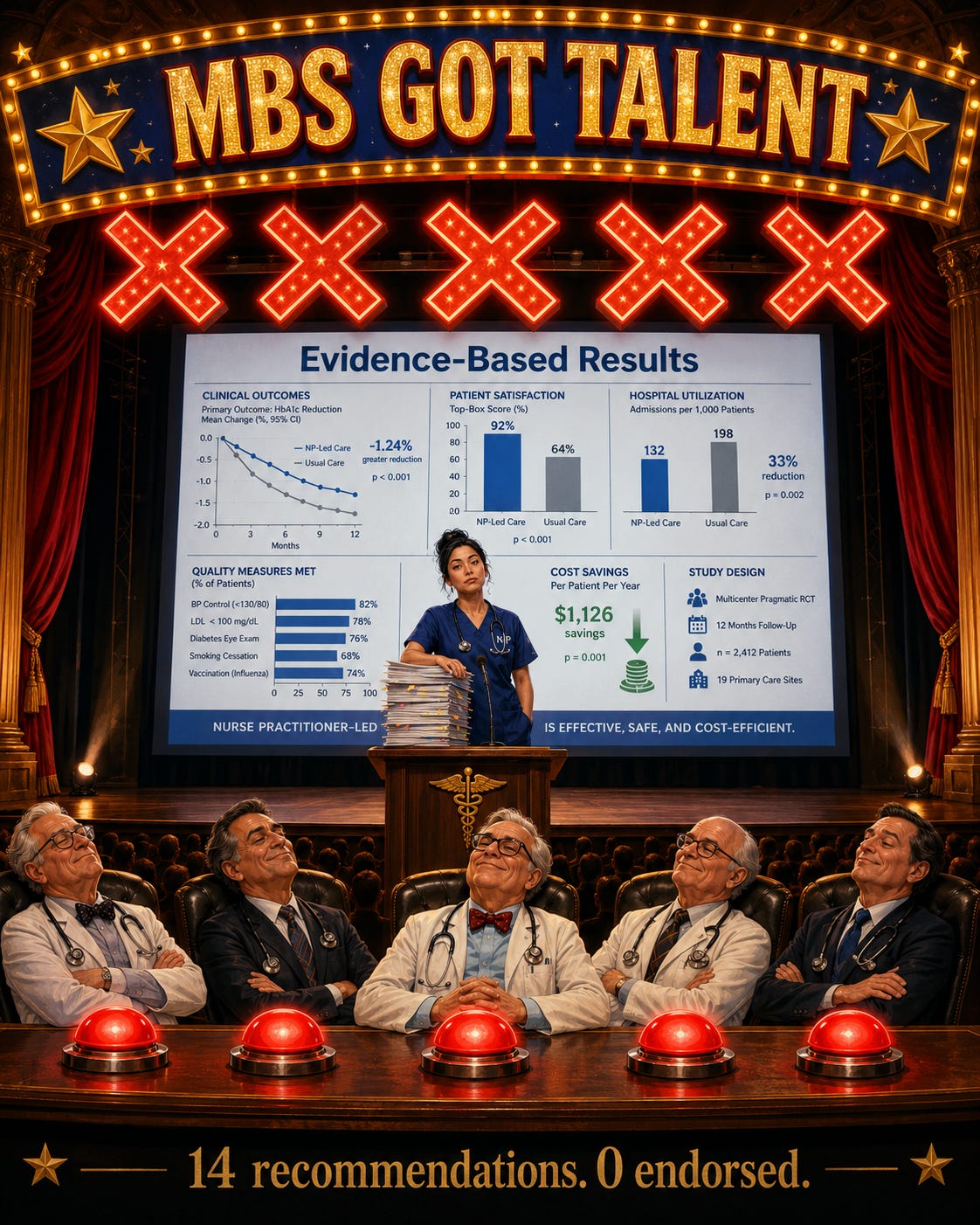
The ACNP kept going anyway, building outcome data governments eventually couldn’t ignore, running the 2023 Nurse Practitioner Workforce Plan through parliament with bipartisan support, and watching the collaborative arrangement requirement finally fall on 1 November 2024 — 34 years after one fed-up nurse backed a health minister into a corner at a conference dinner and refused to let him off the hook.

The AMA and RACGP are still pushing back. The fights over allied health referral rights, MyMedicare enrollment requirements, and bulk billing incentive eligibility are ongoing.
The structural independence of the ACNP is the reason those fights haven’t stopped the profession — because the college can absorb that resistance and keep building the evidence base, without a union’s membership politics pulling it sideways every time the pressure increases.
You’ve done so well to get this point, I’m going to reward you with a not-so-subtle table
…just in case you got lost IATA*.
(in all the acronyms)
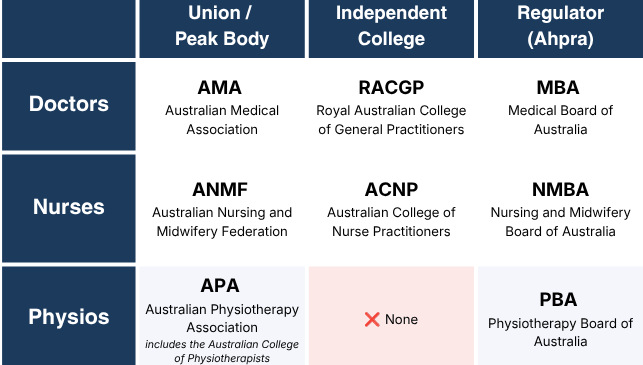
Ok… not-so-subtle point made. let’s get back to Physio-ing.
You cannot do both from the same chair
The APA is simultaneously a union and a credentialing college.
It fights for members’ wages, conditions, and recognition.
It also runs the makeshift-college (Australian College of Physiotherapists) (ACP) with a titling and specialist credentialing framework that is supposed to differentiate the best clinicians from the rest.
These two functions are not compatible.
Solidarity
A union’s power comes from solidarity. The logic is: every member is equally valuable, every member deserves representation, and the moment you start ranking members against each other, you fracture the base. That is not cynicism. That is how unions work. It is why they work.
Exclusivity
A credentialing college does the opposite. It argues, explicitly and externally, that some clinicians are worth more than others. It builds the evidence for that argument. It sets the bar, enforces it, and stands behind it when governments ask: why should we pay more for this person?
You cannot do both from the same chair.
It’d be like the IOC allowing the Athletes Mum to have a say as a judge on their little Timmy’s performance at the Olympics.

The APA knows this, on some level. But it cannot act on it, because acting on it would mean choosing. And choosing would mean someone loses - probably Little Timmy.
Not to mention what it’d also do to the APA Purse.
The Big Tent ate the credential
‘A big tent’ is a political term. It describes an organisation that deliberately keeps its membership criteria broad — accepting as many people as possible under one roof — because its power comes from size and solidarity rather than exclusivity.
Because the APA cannot afford to exclude or differentiate, it accepts everything under the same roof.
Dry needling. Clinical pilates. Wellness. NDIS support work. Hydrotherapy. Criteria-based Non-Surgical management of Achilles Ruptures.
All “physio”. All “equally valuable”.
All eligible for the same Medicare item numbers, the same rebate structure, the same professional identity.

Dry needling is the clearest example — the insertion of a needle into soft tissue, contested evidence base, sits outside physiotherapy scope entirely in most countries or requires a separate credential. In Australia, the APA folded it in, made it a Group, gave it a National Chair, not because the evidence demanded it, because the tent needed to stay big.
The problem is that a big tent and a credible credential are mutually exclusive.
When you tell a government health minister that a:
Titled Musculoskeletal Physiotherapist
working independently at full scope,
reviewing radiology reports (including the images - no just the reports),
screening for rheumatology and other chronic diseases,
liaising with GPs on bloodwork and medications,
taking the lead in third party case management,
whilst applying criteria based rehabiliation frameworks to the non-surgical managment of an ACL rupture to try to avoid unnecessary surgical intervention
….is “more clinically capable” than a general physio, the minister’s next question is reasonable:
“That sounds impressive, but how is that different from the physio doing dry needling and pilates down the road? “

If they’re all in the same organisation, paying the same fees, carrying the same professional identity — the answer becomes very difficult to give.

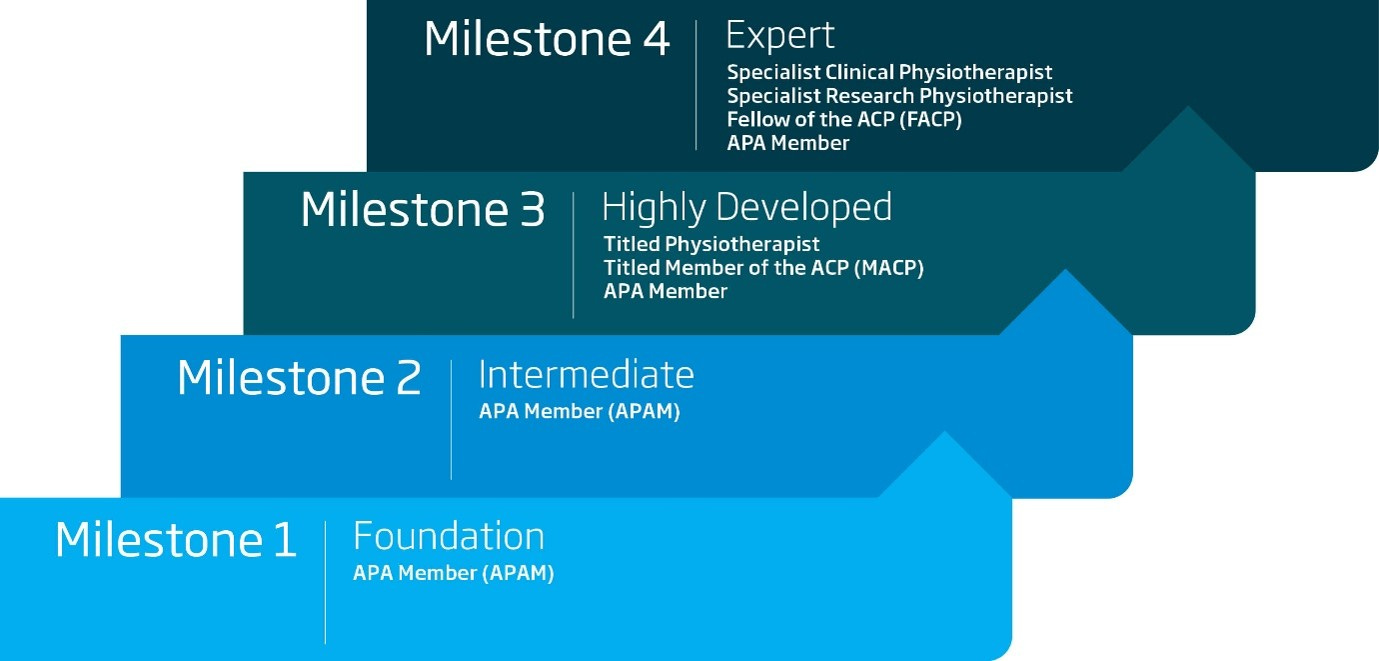
Endorsements vs Specialisation vs General Rego
The AHPRA registration framework has three mechanisms for recognising advanced practice: specialist registration, endorsement, and general registration with an internally issued title.
Specialist registration — a separate registration type with full legal authority — exists for medicine, dentistry, and podiatric surgery.
Endorsement — a formal addition to base registration that confers a protected title and expanded scope — is how nurse practitioners are recognised. It sits on the public Ahpra register, it's granted by the Nursing and Midwifery Board of Australia, and it has legal teeth.
The third mechanism is general registration with a title issued by a professional body. That's physio. No protected title. No register visibility. No legal authority behind the letters.
On the public AHPRA register, a Fellow of the Australian College of Physiotherapists and a new graduate appear identically, under general registration.
The Physiotherapy Board of Australia’s own advertising guidelines require that if a physio uses a specialist title, they must explicitly state it was awarded by the Australian College of Physiotherapists — precisely to avoid the public mistaking it for a statutory credential it is not. [3][4]
Compare that to the Nursing and Midwifery Board’s endorsement table: 3,194 endorsed nurse practitioners with full Medicare access, PBS prescribing authority, and a publicly recognised credential.
One column is essentially blank. The other changed healthcare. [1]
The APA chose solidarity over credibility.
The ACNP chose credibility over solidarity.
Only one of those choices ends with Medicare recognition.
What the profession is actually telling us
On 6 December 2025, a well-intentioned post appeared simultaneously on the APA Musculoskeletal and APA Sports and Exercise Facebook pages. It was a breakdown of APA titling numbers — a pump-up piece, the kind of content that’s supposed to generate momentum.
The numbers: 50,064 registered physiotherapists in Australia as of March 2026. [3] 3,094 APA titles awarded across 14 disciplines. That’s 6.2% of the profession. Roughly 1 in 16.
What followed was not momentum. It was the profession doing a quiet, unsolicited cost-benefit analysis — and arriving at the same answer from every direction.
The $40k comment: “Honestly the thing that held me back from titling wasn’t motivation — it was looking at a $40,000-plus price tag and wondering what I’d actually get for it.”
The “I’d do it in a heartbeat” comment: “For me it’s simple. The day titling comes with real clinical authority — prescribing, direct imaging referrals, expanded Medicare access — I sign up immediately. Right now it doesn’t, so I haven’t.”
The business owner comment: “Running a practice, I can tell you titling doesn’t move the needle commercially. Patients have no idea what it means, and neither do most referrers. A cert from outside the profession would probably do more for the business than an APA title.”
The hiding-the-Masters comment: “I actually leave my Masters off my business card now. I don’t want patients thinking I’m more qualified than my colleagues who went through the proper titling pathway. Meanwhile I’m supposed to pay another $30k for a credential that only other physios recognise? Hard to justify.”
The 25-years-no-title comment: “Did my postgrad MSK dip back in the early nineties. When the professional landscape shifted, my qualification got left in a grey zone the APA never sorted out. I’ve been doing specialist-level work in one area for over two decades. Still no title. Not for lack of expertise — just got caught in an administrative shuffle nobody ever fixed.”
The APA had a target of one third of the profession as Specialists. Current reality: less than 0.5%.
The National Chair of the APA Musculoskeletal Group jumped in and responded in the comments. He’s well known, a great guy, endless energy for bettering not just his patients, but also this trade. He is not a defender of the status quo — his comment is one of the most honest things I have read from inside the profession’s leadership. He acknowledged the cost, acknowledged the gatekeeper concern, and then said this:
“There are active discussions with the APC about having our advanced practice pathways externally accredited — similar to what the nursing profession has done..”
The Chair of the APA MSK Group is pointing toward the nursing model as the answer.
He’s right about the direction.
The argument isn’t with the APA here — it’s with the system they’re trying to reform from inside a structure that cannot reform itself in the way that matters. They’ve been trying it for decades. The weary Physio Vets were right.
The formal research has now confirmed what the thread showed anecdotally.

The 2026 PARC study — co-authored by the APA and the Physiotherapy Board of Australia — found that:
Physiotherapists with further qualifications are more likely to leave the profession.
Not less. The credential didn’t retain them. In many cases it accelerated their departure, by raising expectations the system structurally cannot meet.[5][6]
One participant in the qualitative study put it plainly: “An increase in our scope of practice to treat patients independent of GPs would make a physiotherapist want to stay in physiotherapy for 40 years.”[6] Yes. Yes it would.
And geeze louise…. patients (and many GPs) are just begging for us to have that autonomy.
The Army and the SAS.
I served in the Australian Army.

The regular army was large, reasonably equipped, and sent to reasonably manageable situations. We got okay pay, okay gear, and okay outcomes. That was fine. That was the job.

But then there were the Special Forces. Smaller. Trained harder. Sacrificed more. Paid more. Better equipment. Better missions. Better outcomes.

And they were not embedded in the regular army pretending to be the same thing — they had their own structure, their own selection process, their own reporting lines, their own relationship with government.
Now imagine there was no SAS.
Imagine those elite soldiers were just... in the regular army. Training harder than everyone around them in their own time. Staying back at the base while their peers went to the pub. Fine-tuning navigation and close-quarters skills on their weekends. When they deployed, there would be one elite soldier to every nineteen others, doing most of the clinical work, on a standard ticket.

They would leave. They’d probably go overseas to another special forces unit.
Not because they stopped caring about the Australian Army. Because the structure gave them nowhere to go.
That is the titled or specialist physio in Australian physiotherapy right now.
Genuinely better. Doing more demanding work. On the same item numbers as the new grad in the next room. The career pathway doesn’t exist. The external recognition isn’t there.
The Special Forces community is independent of the regular army in how it proposes things to government for funding.
That independence is not incidental.
It is the point.
Internal titles meant everything to physios and nothing to anyone else
The facebook thread confirmed it. The research confirmed it.
The only people who understand what an APA title means are other APA members. Patients don’t know. GPs don’t factor it into referral decisions. Medicare doesn’t differentiate. Insurers don’t pay more for it.
As one of the experienced physios on that Facebook thread put it: “…getting a certification well known outside of physio might be more commercially useful than an APA title.”
That is not a cynical observation from a disengaged clinician. It is a rational assessment from someone finishing a Masters pathway and reconsidering whether the system is worth it.
The APA’s position, when pressed on this, has been that “the profession hasn’t done a good job explaining titling to the public.”
So they bang the same old drums outside federal parliament some more.

And then they head to the states and territories.

But nursing didn’t solve the public recognition problem with better marketing.
They solved it by building a structure that gave external bodies — governments, hospitals, Medicare — a formal mechanism to recognise the credential.
You can explain an internally issued title forever. Or you can build the thing that makes external recognition structurally possible.
Physio had a spark. It was put out.
This is not a new problem, and the APA is not the villain of it.
We have our own Origin Story too - not as cool as ‘Tipsy Fed-Up Nurse Bails Up the Politician at the Conference’, but it’d be rude if I didn’t acknowledge it.
We lit the Spark before the Sisters.
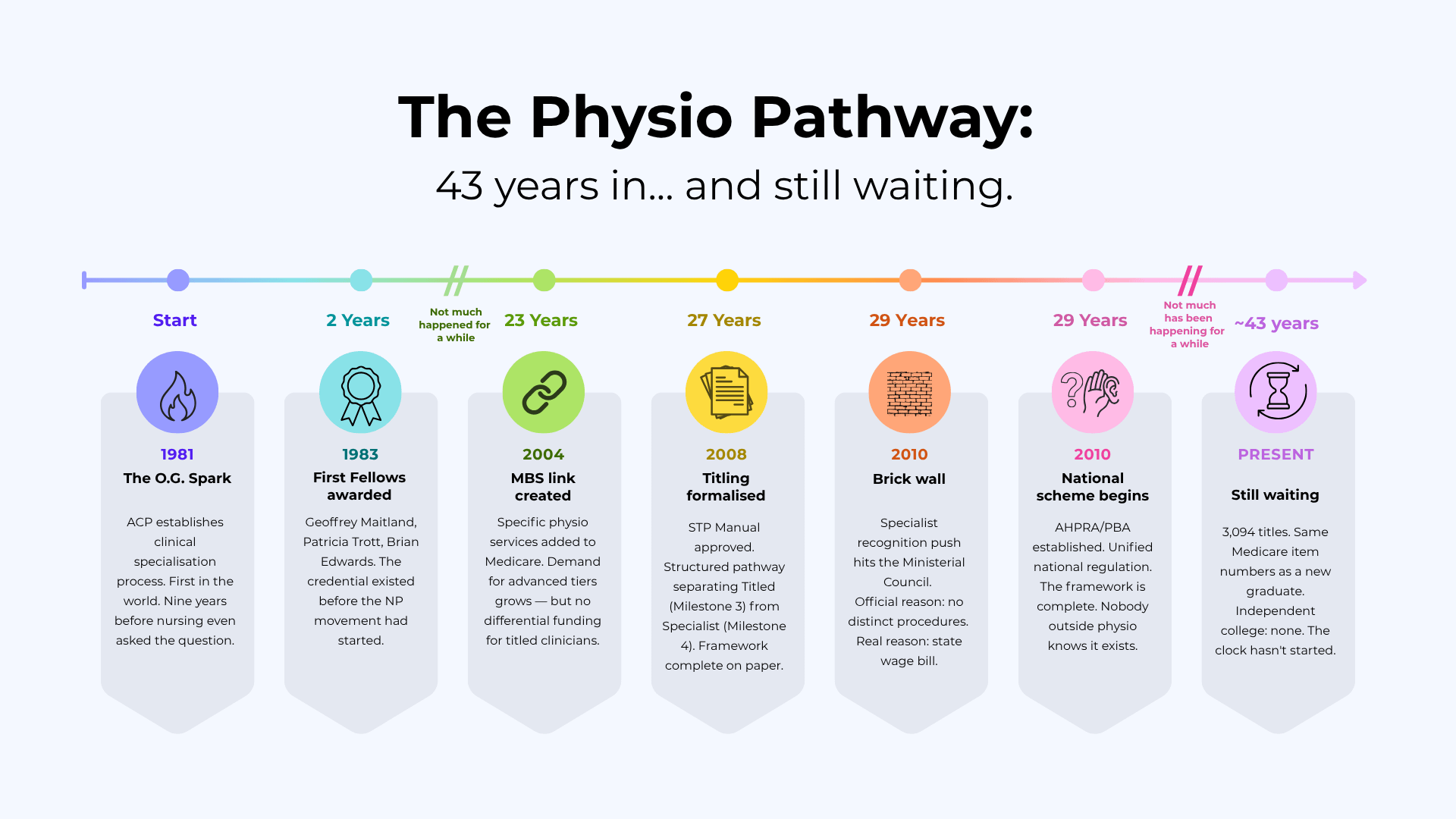
In November 1981 — nine years before a nurse at a Sydney conference asked a health minister a pointed question — the Australian College of Physiotherapists formally approved the clinical specialisation process. [7]
In 1983, the first Fellowships by Specialisation were awarded to Geoffrey Maitland, Patricia Trott, and Brian Edwards. [8] It was a big movement for the trade.
Maitland in particular was quite adept at Pushing for good ‘Movement’ outcomes.
(incredibly niche trade joke)
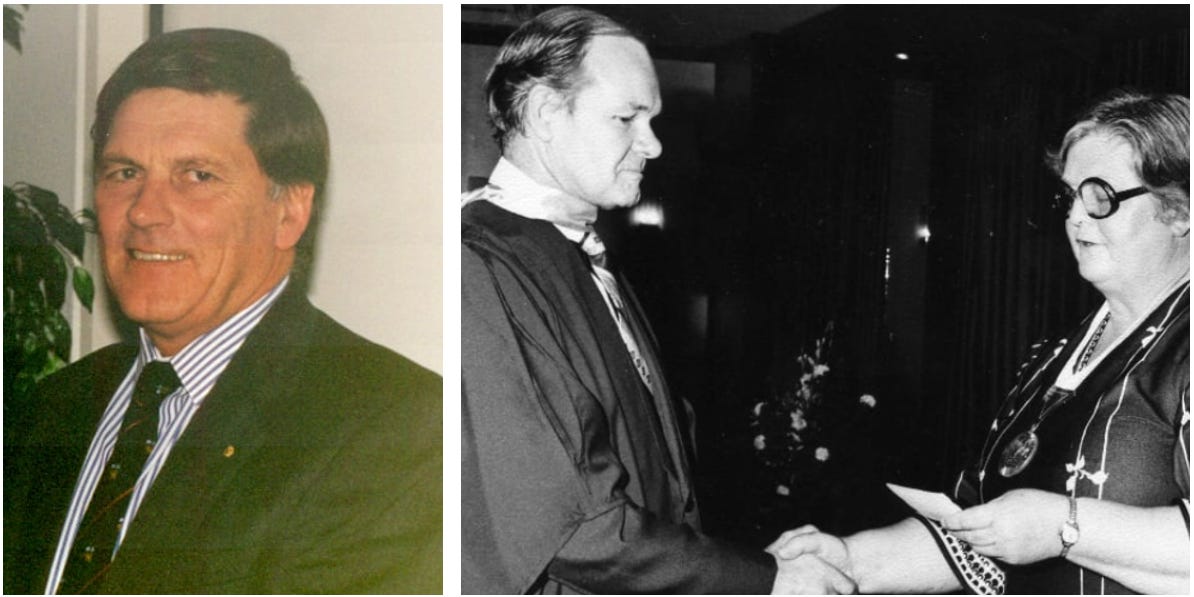
The credential existed before the NP movement had even started.
By 2008, the Specialisation Training Program Manual had been formally approved, creating a structured registrar training pathway. [9]
By 2010, the National Registration and Accreditation Scheme commenced, establishing AHPRA and the Physiotherapy Board of Australia — and with it, a unified national framework that should have provided the architecture for specialist recognition. [10]
It didn’t.
In the lead-up to the 1 July 2010 commencement of the National Law, the Physiotherapy Board applied for specialist recognition through the Ministerial Council — Health Ministers from each state and territory.
The Council deferred it. [11]
The official reason given was that physiotherapists had no distinct procedures that warranted a specialist classification.
But the inside goss, from people who were in those rooms, was a line item on a state health budget:
Specialist recognition would trigger reclassification of government-employed physiotherapists, and Health Ministers from smaller jurisdictions weren’t prepared to wear that cost.

The spark went out.
And unlike nursing, physio had no independent body to keep the fire going.
In NP terms, physio’s specialisation story started nine years before nursing’s — but without the independent college structure nursing built in 2003, the credential never travelled beyond the profession’s own walls. Nursing built the structure. We built the framework and left it in a drawer.
The NPs at Year 15 had an independent college. We’re at Year 43. We still don’t.
Full PDF download of those timelines available at www.physioclinician.com.au/blog
The direction is right. The structure still isn’t there.
Something has shifted very recently that is worth acknowledging.
The Physiotherapy Board of Australia is developing a proposal for an endorsed prescribing pathway — physiotherapists who complete a Board-approved program gaining the authority to prescribe medicines. A working group is reviewing the risks and benefits. More information will come.
This is the right direction.
An AHPRA endorsement with legal authority. A Board-approved program. Formal credentialing that external bodies can verify and trust.
This is structurally different from an APA title. This is what matters.
But there is a question embedded in that working group’s membership that deserves to be asked plainly:
if the APA is in the room as a credentialing participant rather than purely as a membership advocate, the structural conflict of interest hasn’t been resolved — it’s been moved upstream.
The NP story shows what happens when the body that represents members is also the body that designs the credentialing architecture. You get 14 years of collaborative arrangement requirements that everyone acknowledges are a barrier and nobody removes because the political cost is too high.

The Board’s own PARC research — co-authored with the APA — recommends exploring “the role of endorsements on national registration to recognise postgraduate qualifications and advanced skills with higher grade levels, similar to nurse practitioners.” [4]
The institutional consensus is forming. The direction is clear.
The structural question is whether the vehicle being built will be genuinely independent, or whether it will recreate the dependency problem nursing spent a decade dismantling.
The close
The December 2025 APA Facebook threads were also full of “it’s not about external recognition, it’s about you being the best you can be!”.

Being a better clinician is a noble pursuit. Nobody is arguing against it. But ask the nurses. They had clinicians training harder than everyone around them, staying late while colleagues left for the pub, fine-tuning their skills in isolation.
And it changed nothing systemically until they built the independent college.
Individual excellence without structural recognition is unpaid overtime with better clinical reasoning.
You cannot fix the trade by fixing the individuals. You fix the trade by building the thing that makes individual excellence externally visible, externally verified, and externally rewarded.
Nursing did this. It took 34 years.
It required one structural decision in 2003 that physio still hasn’t made and yes, it was painful.
The prescribing proposal is a step. The PARC research is an acknowledgement. The MSK National Chair’s facebook comment is a signal. The December 6 thread is a reckoning that was never meant to happen in public.
The clock only starts when the structure is built. Not when the marketing improves. Not when the universities stop issuing confusing entry-level doctorates. Not when advocacy gets louder.
When the structure is built.
Physio needs a Sister Act.

References
Previously:






If this saved you wading through the literature yourself, subscribing funds the next deep-dive.
Or shout me a Blog-Typing-Juice at:


{kind=link}
Not every post is for everyone.
Substack lets you filter which sections you get emailed. Hit “Manage Subscription” in your account, or click “unsubscribe” at the bottom of any email (it won’t kick you out immediately — it gives you the choice).
The four streams:
Patient’s Playbook — Plain-English guides for patients and parents
Clinician’s Corner — Clinical reasoning, case studies
Research Reviews — Papers and guidelines, dissected
Clinician’s Compass — The state of the profession
Pick what suits. I won’t take it personally.