
Clinician's Corner | Case Study: Stiff and Sore Elbow - Smoke on MRI, Fire in the Scope
A case study featuring synovitis, missing radial head real estate, hidden loose bodies… and an Indiana Jones-type cave made of scar tissue.

Before we dive in, a note: this case is shared with full patient consent, including pictures of their ‘loose bodies’ extracted from their elbow during the operation which I had the privilege of observing. Thanks also to the Surgeon, their team, and the theatre staff for having me.
The first part of this post is an introductory preview—the valuable clinical insights, practical recommendations, and expert guidance are behind a paywall for paid subscribers only.
If you find my free content helpful, becoming a paid subscriber gives you:
✅ Full access to expert-backed strategies and pain management insights
✅ Direct access to me via subscriber chat—ask me questions anytime
✅ Ongoing, high-value information normally provided in a clinic for hundreds of dollars
This post is a guide only and should not be taken as medical advice. It does not replace assessment and recommendations from a registered and regulated healthcare professional.
Some elbows age quietly.
Others age like a dial-up modem exposed to a Canberra winter — slow, stiff, and one small stress away from complete meltdown.
This is a story about the second kind.

The Case: The Bent, Grumpy Elbow That Wouldn’t Behave
A 50–60-year-old very active and adventurous gent came to see me with a non-dominant elbow that had recently gone from “stiff but fine” to “I can’t even touch my face”.
As always, 90% of the public (and half the health system) default to calling any elbow pain “tennis elbow”. But this clearly wasn’t that.
Important bits:
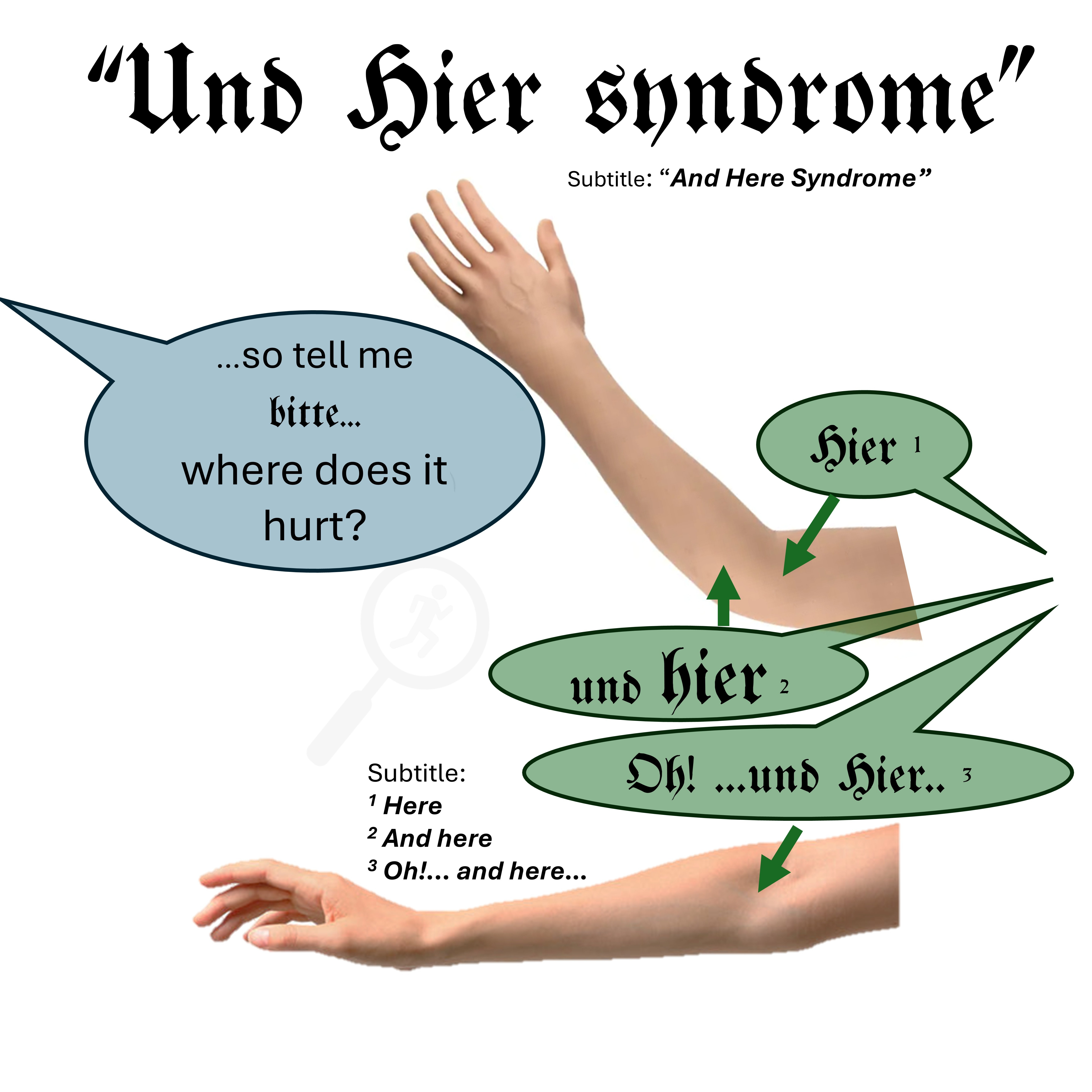
Old fracture decades ago → radial head + capitellum involvement.
Always been a bit stiff, but not symptomatic.
Suddenly:
Loss of extension (first sign)
Then loss of flexion (couldn’t touch his face easily)
Grip strength painful but not convincingly lateral tendinopathy (grip painful… but strong)
Achy inflammatory pattern, worse later in the day, often at night
Global elbow pain … posterior, laterally, and inevitably anterior… which is clinically when you know things are “pretty far gone” if it isn’t a distal biceps tendon issue.
So the patient had a moderate elbow case of “Und Hier Syndrome”.
Every part of the story so far pointed at a joint-driven, not tendon-driven, pathology.
So my clinical picture was screaming: “the joint is cranky and inflamed” (capsular inflammation/synovitis)
From here on, I may (or may not) have leaned far too heavily on references to a very famous adventure-movie hero. My team of entirely hypothetical lawyers has strongly advised that, to avoid attracting the attention of one of the world’s biggest movie studios (let’s just call them Dalt Wisney), I should make things obviously, unequivocally different.
So allow me to introduce the Healthcare Warrior who lives rent-free in my mind:
Doctor Montana Joans.
Because an adventurer-type patient absolutely deserves an adventurer-type narrative.
Dr Joans is part Clinician (in the early stages of this case), and part Surgeon (in the latter stages… when it’s very clearly not the Physio holding the scalpel… natürlich).
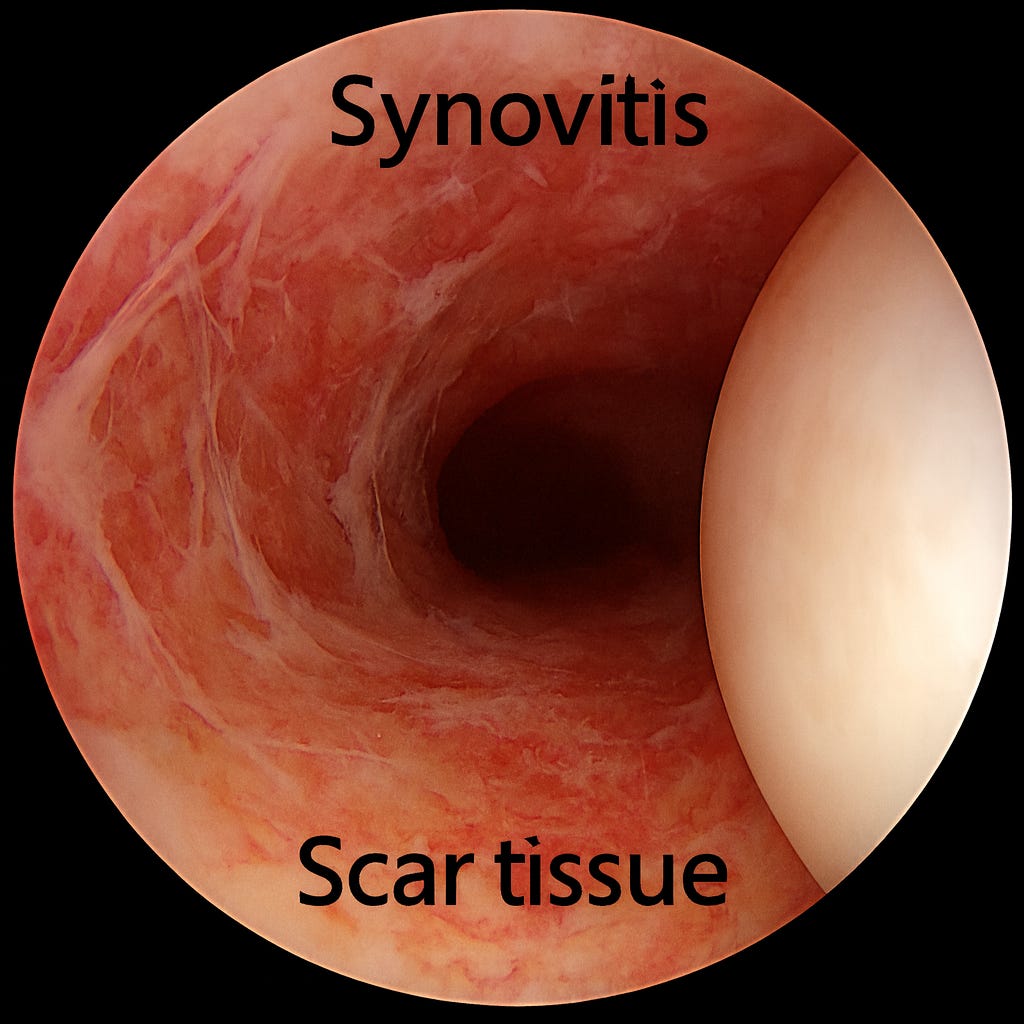
However before we commence our short but epic clinical journey, I’d like to acquaint you with what a calm joint looks like in my mind (and also on the arthroscopic camera):

und jetzt… here is what a Cranky and Inflamed joint looks like:
Initial Management: Anti-inflammatory

We trialled:
2–4 weeks anti-inflammatories
Cutting out all weight-bearing (“avoid push-ups”) and loaded extension (“avoid tricep dips type movements”)
Eliminating other aggravators (eg: boxing, planks, push-ups)
Monitoring Range of Motion (ROM) + grip strength
Functional ROM (“can you touch your face yet?”) as well as ROM objective measures.
Grip Strength utilising a Handheld Dynamometer
Montana trials an oral NSAID.
He improved, but only partially.
Then… regressed again with very little provocation.
That’s the thing with a truly cranky joint:
Push it, and it pushes back harder. Nicht sehr gut!
Diagnostic Imaging: Lots of Smoke, No Clear Fire
Given the traumatic history (radial head and capitellum impaction fracture), XR referral was first, followed by an MRI shortly after.
🔒This is where the free preview ends. Paid subscribers now get access to the full post, including the clinical pearls, key takeaways, and practical recommendations.
