

Clinicians Corner | Saving the Unhappy Kneecap Joint
Evidence-Based Management of Patellofemoral Pain

Evidence-Based Management of Patellofemoral Pain
This post is an introductory preview—the valuable clinical insights, practical recommendations, and expert guidance are behind a paywall for paid subscribers only.
If you find my free content helpful, becoming a paid subscriber gives you:
✅ Full access to expert-backed strategies and pain management insights
✅ Direct access to me via subscriber chat—ask me questions anytime
✅ Ongoing, high-value information normally provided in a clinic for hundreds of dollars
This post is a guide only and should not be taken as medical advice. It does not replace assessment and recommendations from a registered and regulated healthcare professional.
Main Points:
Patellofemoral pain (PFP) occurs mainly in active people who usually have increased their ‘up & down’ demands too fast-too soon.
It’s key to educate PFP patients in what causes the increased loads on the Patellofemoral Joint (PFJ) and help keep them active throughout the week whilst dialling back ‘up & down’ tasks.
Management of PFP can be made much easier by assessing Pain-Free Knee Extension Force Production (“quads strength”) and correlating it to the patients body weight and also uninjured side.
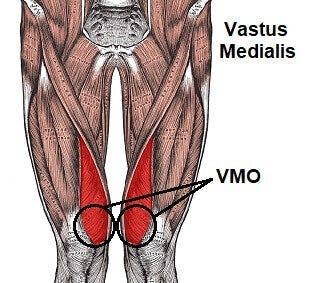
There has been an over-emphasis on isolated VMO strength, ITB “tightness”, isolated Hip Abduction strength, Knee Valgus, “Patella Maltracking”, and Foot “over pronation” over the past 20 years.
Rehab should focus on increasing the contact area between the patella and the femoral trochea in order to reduce joint load — this is best achieved via knee extension force production (aka Quads Strength).
It’s a typical day at the clinic.
We typically treat the typical active population, who get the typical knee pain, which I had previously typically treated with typical interventions and exercises typically recommended by typical research.
…well … until 2020 (the year when everything went haywire in the world) when I started treating typical knee pain, atypically.

Here’s the:
Typical Patellofemoral Pain Patient
The 20–40 active person comes in with tight knees and discomfort, perhaps an ache after working out, but it doesn’t stop them. It’s getting worse or they’re fed up. Perhaps their knees are noisy.
This person has a history of having a week full of one or more of the following: jumping, squatting, running (especially with hills), or playing a sport with a variety of those….they generally go “up and down” a lot.
There’s no history of direct trauma. They’ve tried stretching, foam rolling, massage guns, trigger points any anything else that was recommended by their gym-going peers or their search on the internet but to no prevail.
They may or may not have had received the usual “advice” that: “noisy knees means cartilage damage” “their patella is mistracking” or “maltracking”, “they have a weak VMO and/or a tight ITB”.
They may or may not have XR/MR imaging that reports “wear and tear/degeneration/osteoarthritic changes”.
On physical assessment there’s no deformities/abnormalities, they move normally, their foot posture is not outrageous — they are not “rolling in” significantly.
There’s mild to moderate pain with hopping, jumping and big step ups.
There’s mild to moderate pain with (usually 50–80%) isometric knee extension strength (basically kicking their leg up against an immovable object).
They have full knee range of motion, no pain along the joint line of their tibiofemoral joint (aka ‘The Main Knee Joint”), no history of instability, buckling or posterior knee pain.
On palpation (which is ‘science’ for: touching their bits) they usually have pain around the patella/kneecap.
We’ve ruled out (or don’t yet suspect) the following: patella dysplasia, recent/acute patellofemoral instability episode (subluxation/dislocation), any other recent trauma such as landing on the kneecap area, patella tendinopathy (which is actually very uncommon outside of an elite sports environment, unless they are a regular jumper of some sort). We don’t suspect fat pad involvement (also uncommon, but usually short-term if managed well) and we’re fairly sure the tibiofemoral joint (main knee joint) isn’t involved as there’s full range of motion there.
PAUSE THE SCENARIO!
What do you think? What do you tell them? What do you do to them? What do you recommend they do to themselves? What has the research told us over the past 20 years and how do we apply it?
That there, my friends, is the current challenge of Patellofemoral Pain (PFP), pain which refers from the Patellofemoral Joint (PFJ)
Runners Knee, Patellofemoral Pain Syndrome, Patella Mistracking Syndrome, Anterior knee Pain, Anterior Knee Pain Syndrome, Patella OuchyWouchy Syndrome… whatever you call it, managing an overcooked patellofemoral joint (PFJ) is a challenge.

11–17% of knee pain presentations to GPs relate to PFP (Van Middelkoop, Van Linschoten, Berger, Koes, & Bierma-Zeinstra, 2008; Wood, Muller, & Peat, 2011), and in a sports clinic setting roughly 1/3 of knee pain cases relate to PFP (Kannus, Aho, Järvinen, & Nttymäki, 1987; Taunton et al., 2002). When it comes to kids, 6–7% of the adolescents will get PFP (Mølgaard, Rathleff, & Simonsen, 2011; Michael Skovdal Rathleff, Roos, Olesen, & Rasmussen, 2015), but as will be outlined in this blogpost PFP occurs more often in active people, particularly those doing more jumping and ‘vertical tasks’ (hills/stairs), 16% of adolescent female basketballers for example (Myer et al., 2010).
There’s a bit more going on than “TIGHT ITB and WEAK VMO”, which is “tHe CAuSe oF aLL KneE ISsUeS!?” according to those who aren’t health professionals or those who are health professionals but lack the time to explain complex health conditions to patients and manage them well.
On a recent BJSM podcast it was raised as the “low back pain of the lower limb” as a statement on how little we still know about it and the challenges in managing PFP. There are so many potential nociceptive structures (things that can cause a nociceptive stimulus into the brain, the output of which is: pain) around the PFJ: Hoffas Fat pad, Patella tendon, Patella capsule, MPFL, VMO, ITB, Patella Bone, Tibial Tuberosity, Anterior Tibiofemoral joint referral… and much more.
There has been a lot of interest in the management of PFP in the past 10 years. We are fresh off a decade-long ‘bandwagon’ of suspecting “tight ITBs and weak VMOs” were causing a “patella tracking” issue… before we realised that there was more pain-free and happy people with “patella maltracking” on imaging than painful people, therefore it must be quite a normal variation (similar to the “ankle/foot pronation is a villain” narrative, which popular shoe stores still use to upsell expensive shoes).
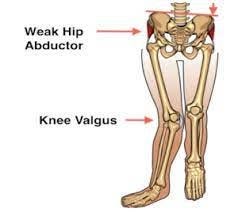
After we tracked away from maltracking and “foam rolling (or stretching) all the tight ITBs” (which was implausible to begin with) we moved onto Gluteus Medius as primary driver of PFP, because it shares a role of lower limb stability to avoid knee valgus (have a drink every time ‘valgus’ comes up in this post, I dare you!). Glute medius being an active force (70%) to resist dynamic valgus, and ITB/TFL being a passive restraint (30%.. or so we’re told).
I started to suspect there was more to managing this condition than the above, and that hunch was confirmed once I read an in-depth blog on this condition at the www.painscience.com/ website by Paul Ingraham which spelt out what is assumed now to be ‘Fake News’, or put more subtly, misinformation/misunderstanding of the research. A great chat between Dr Bradley Neal and Greg Lehman on episode 48 of The NAF Physio Podcast discussing patellofemoral pain and knee biomechanics highlighted that we simply don’t know what’s cause and effect in the PFJ, particularly when it comes to hip adduction/knee valgus.
For me, management involving activity modification and education of this condition is crucial as patients can do as much foam rolling or stretching as they like however if they are still doing a high amount of ‘up and down’ activities in the week they’ll get nowhere.
Who is the Typical PFP Patient?
20–50 years of age
Fairly active throughout the week — likes to run, jump, hop, do gym glasses, do weights, play sports.
Has Anterior (front of) knee pain
For the purposes of keeping this blog as short as possible, the following needs to be also considered however let’s assume the above ‘Typical Patient’ doesn’t have them:
A recent history of instability (subluxation/dislocation)
A recent history of landing on the kneecap (contusion)
Localised patella tendon pain (should be a regular athletic jumper if they do)
Patella Dysplasia (including patella and trochlea dysplasia and patella alta etc)
Younger pathology such as an active Osgood Schlatters/tibial tuberosity apophysitis pain
The PatelloFemoral Joint
Oh boy, this is a beautiful joint. I don’t know why I like it so much, it’s just… odd and complex…yet simple.
The role of the PFJ is to hold you up (stop the knee from buckling) by producing a knee extension force. Knee extension is pivotal in kicking and jumping sports and is especially challenged by up/down tasks such as incline running, heavy squats and jumping.
The key components of the PatelloFemoral Joint are:
The Patella bone and the Femoral bone…thus ‘patellofemoral’ (….. get it? these science boffins sometimes good at naming stuff!)
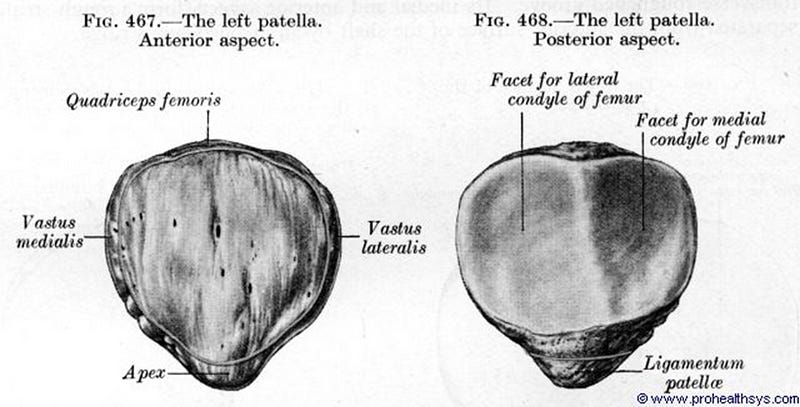
The Patella (Patello-)
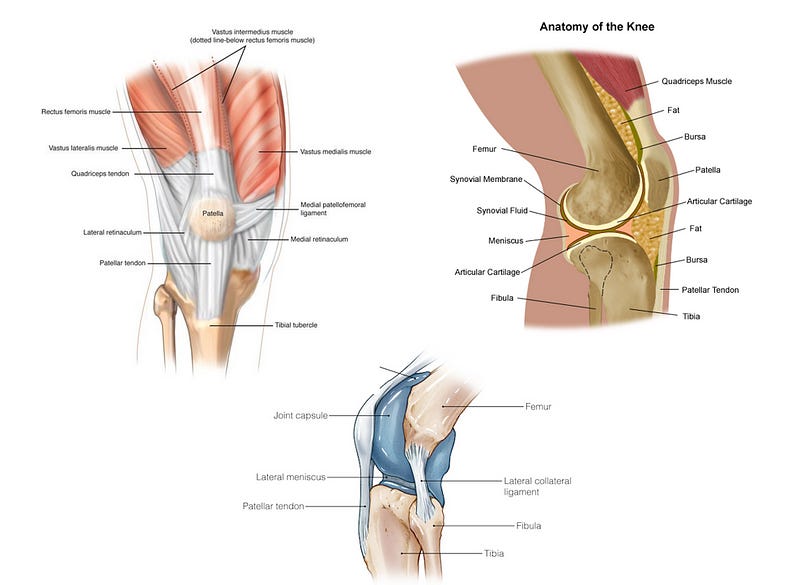
..is a floating bone suspended inside a tendon (quadriceps tendon), there’s even some fibres that are continuous through the bone which is amazing. It has two facets (flat surfaces), a medial facet (toward the body midline) and a lateral facet (away from the body midline). The lateral facet tends to take more load and demonstrate degenerative changes earlier in active people. The facets are covered in articular cartilage which help protect the bone of the patella. The patella, if viewed from above (caudal view) resembles a triangle, which fits nicely in the triangle groove of the Femoral Trochlea. This ‘nice fit’ is called ‘joint congruency’ and it’s really important for happy joints that are put under load regularly. This lovely colourful pic gives a nice representation of ‘spread of joint surface interaction’, which I discuss later.
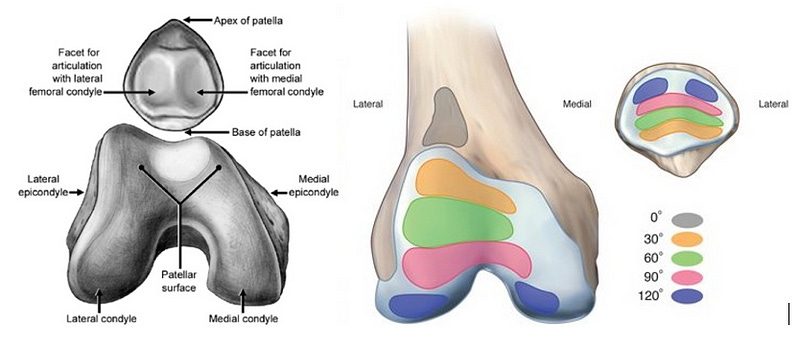
The Femur (-femoral)
..is the distal or far end of the biggest bone in the body forms the top part of the knee complex. The patella fits nicely in a groove called the ‘Femoral Trochlear Groove’, which sits between the two big ball shaped bits called the ‘Condyles’. As the colourful picture shows, the Patella glides up and down the Trochlear Groove depending on the position of the knee (different degrees of flexion). As we’ll find out later, the better the fit (joint congruency) of the patella into that groove and the more the two surface areas remain in touch the more comfortable patients with PFP are (in the absence of trauma and focal articular cartilage loss).
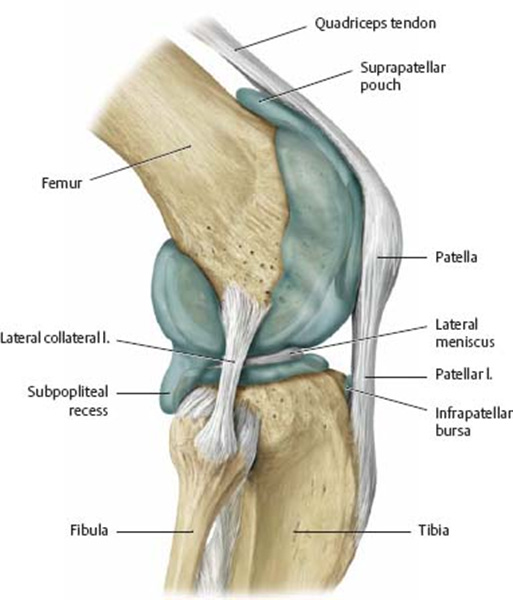
There’s a joint capsule (shown in blue above). There’s not much chat about joint capsules but they might be one a contributor to nociception around the PFJ.
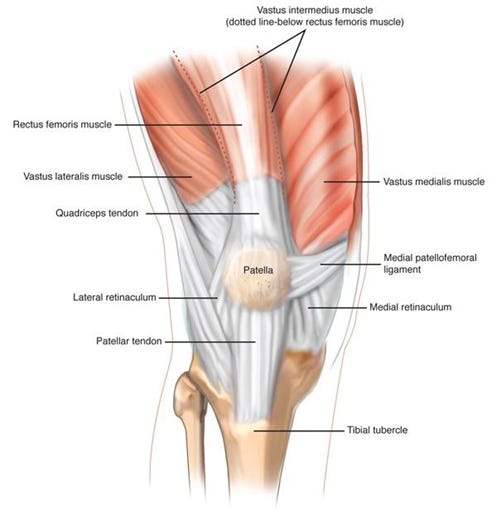
Finally, there’s a whole bunch of soft-tissues and ligaments which help stabilise the patella in the PFJ. Including the medial retinaculum MPFL (medial patellofemoral ligament, usually torn or ruptured during PFJ instability episodes) and the infamous VMO and VL/ITB complex.
What does the PFJ do? What Loads it?
Apart from holding you up when you’re upright and stopping your knee from buckling under your body weight, as a part of the quadriceps-knee extension complex, the PFJ helps you go ‘up and down stuff’.
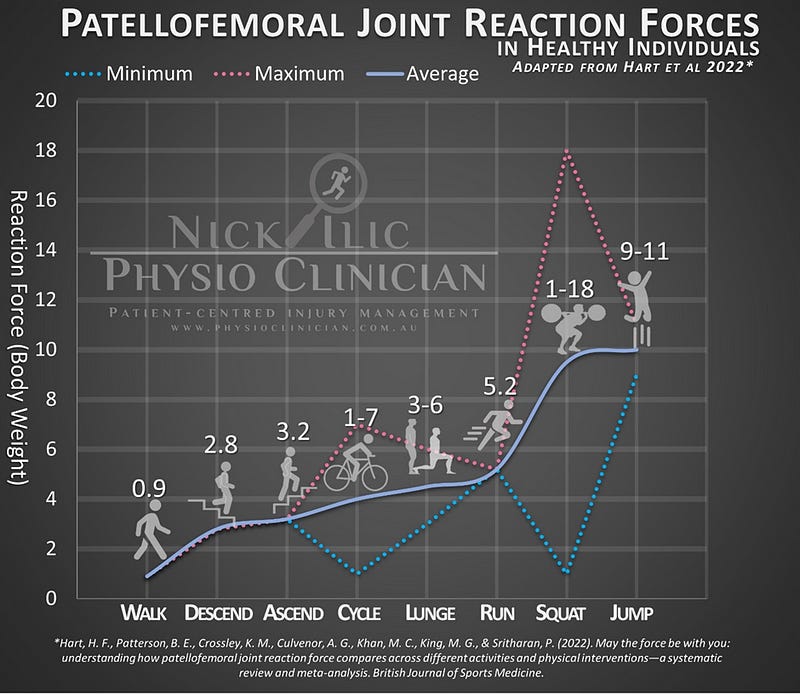
A recent study (Hart et al., 2022) gives some does data on what loads the PFJ. This is shown in my graph adapted form the study below.
The more force (or mass… or acceleration ….. yes…. F=MA) the more the PFJ load.
The Hart study suggests that the PFJ is loaded with tasks that
1. Have a high quads demand, and
2. Are in deeper knee flexion
The Pain
I have previous discussed the hip joint and how we often get ‘join referred pain’ into common but vague areas. The PFJ is similar in that it is often extremely difficult to be specific about what is causing the pain. However there are some studies which have a crack:
A 2011 paper (Farrokhi, Keyak, & Powers, 2011) creatively and fortunately titled “individuals with patellofemoral pin exhibit greater patellofemoral joint stress” surprisingly found that … (wait for it) individuals with patellofemoral pain exhibit greater patellofemoral joint stress!
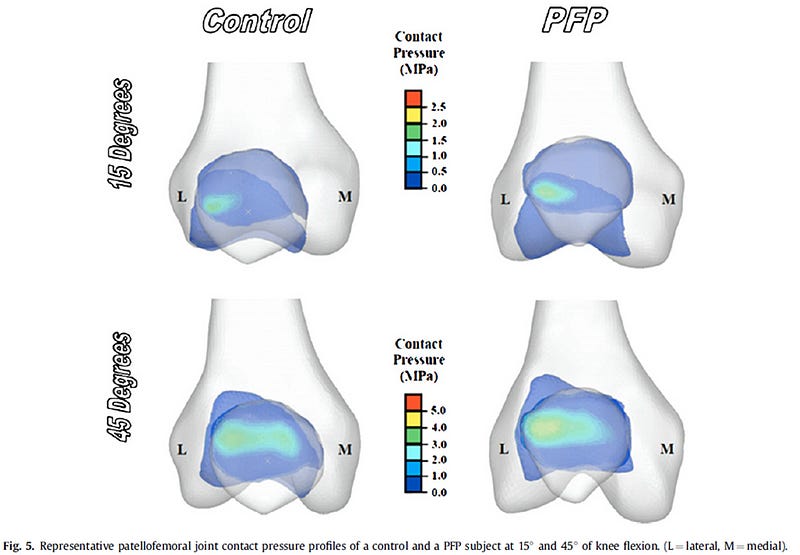
However, … it’s chicken or the egg…. Does pain change the way people move and function, or does the way people move and function change the pain? So what causes the pain? These authors suggest the increased hydrostatic pressure of the joint fluid could stir up the bone-cartilage (osteochondral) interface.
Two Docs do something Dodgy
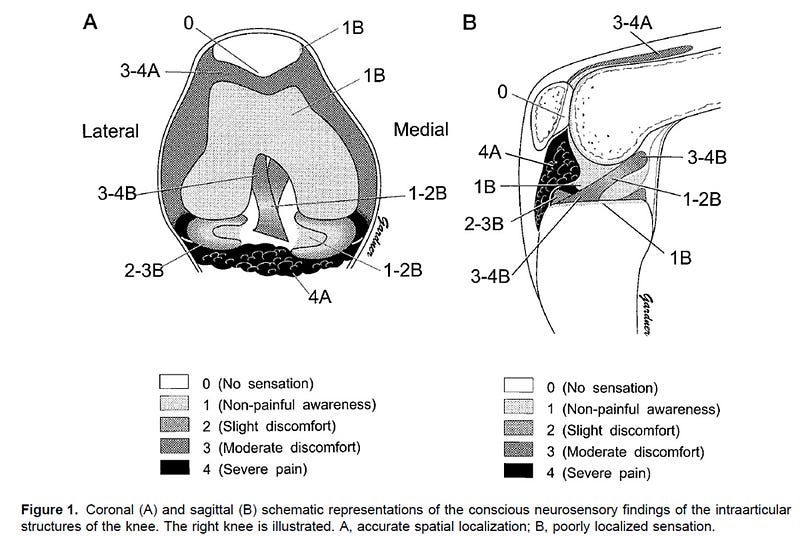
Let’s probe further into what could cause pain in the knee by talking about one very cool study (albeit n=1 study) (Dye, Vaupel, & Dye, 1998)that might not pass an ethic committee today.
A Surgeon and his Mate (also a surgeon) were sitting around drinking one night when he said to his mate:
“Hey! What if you cut open (arthroscope) both of my knees and poke (with a spring loaded device with a 3mm tip) and all around the knee and kneecap joints (with 300–500g of pressure) and see what hurts and what doesn’t!”
To which his mate said:
“Shit yes! Let’s do that!”
(Legal disclaimer: This conversation may or may not have happened this way, I just like to think it did)
So a 46yo Dr Scott Dye had both his knees scoped by his mate Dr Geoff Vaupel and they poked all around the joint and this is what they found to be painful (scale 0: nothing, 4: very ouchy):
This is the sort of stuff that deserves a Nobel Prize ala Australian Dr Barry Marshal winning a Nobel Prize for swallowing gastic ulcer-causing Helicobacter Pylori bacteria.
For the past several years I was thinking that a distension of the joint capsule due to increased fluid inside the PFJ may contribute to that vague feeling of “tightness” around the joint, however I’ve recently pulled back from that idea in favour of the feeling of tightness and other symptoms being a ‘non-specific joint referral’, I’ve written more about ‘Non-Specific Joint Referrals’ here.
Self-Limiting
Unlike the tibiofemoral joint (or the “main knee joint”), the PFP is “self-limiting” in that it resolves over time, and those who have it can (and do) push through a fair bit of discomfort and it often doesn’t stop them doing tasks until it gets really stirred up.

However, just because it doesn’t stop the patients doesn’t mean they aren’t affected. A 2 year follow up of adolescents with PFP found that a quarter of them had PFP over that 2 years and it affected their performance in sports and also their quality of life (Michael S Rathleff, Rathleff, Olesen, Rasmussen, & Roos, 2016). Clinically, we see many adults in their 20s and 30s who suffer have suffered from PFP for years, many report they arrive reporting a “lifelong disability” affecting their knees making stairs/jumping/squats activities very uncomfortable (at best) and painful (at worst). Fortunately the majority of these have simply been mismanaged (ITB stretches and isolated VMO exercises probably) and have potential to settle.
Some patients have developed a irrational fear about the sounds and feelings around their knees, especially the Crunchy or Clicky knee:
The Crunchy Knee — Patellofemoral Creptius
The Wonderful Claire Robertson, aka ‘Claire Patella’ who is a UK Physiotherapist has some fantastic resources on Cracking or Crunchy knees which we call ‘Crepitus’.
The summary is, you can have noisy knees without pain, you can have quiet knees with pain and you can be anywhere in between, but you shouldn’t let your noisy ‘crunchy’ knees worry you if you are active and not getting too much Patellofemoral Pain, it’s not necessarily a sign of joint damage. See an experienced registered healthcare professional for assessment if you have concerns.
For more on this, here is a nice blog on Tom Goom’s (Running-physio.com) webpage by Clare: https://www.running-physio.com/crepitus/
What have we been doing about it the last 20 years
Patella “Maltracking”
A quick search on google will suggest you have a “tight ITB” and/or a “weak VMO” which may be causing “patella maltracking” and you need to “lengthen your ITB” with foam rolling or deep tissue massage and “strengthen your VMO” with VMO exercises.
You can use ‘McConnell Taping’ to pull the kneecap back across so it’s ‘in alignment’ (*SHUDDER*.. I hate that word). However, there may be some other reasons why McConnell’s taping works and it has nothing to do with pulling it medially… but more to do with compressing the patella back into the groove, or getting as much of the two joint surfaces in touch with each other, Mike Reinold has a nice blog on that here.
All of the above “Patella Maltracking from tight ITB and weak VMO” is simply an outdated concept (for insidious onset PFP in the absence of trauma and instability) and yes even I was doing this ‘patella maltracking’ stuff back in the mid 2010s. Everyone was on a foam roller and doing isolated VMO exercises in my clinic. Fortunately I’ve unlearned and evolved as a Clinician.
So is it just quads weakness then?
So if it isn’t VMO it must just be weakness of the Knee Extensors (quads) as a group that causes PFP, that’s just commons sense right?
Perhaps.
For a while there I was testing knee extension “strength” of my PFP patients and if the affected knee was weaker I’d say:
“AH HA! Weak Quads, that’s why you have PFP!”

But then one must consider two words, which can be simplified into four words.
Arthrogenic Inhibition, …..or “OUCHY JOINT, WEAKY MUSCLE”
‘Arthr’ = joint, ‘genic’ = from there, ‘inhibition’ = unable to work normally… so the joint is causing nearby things not work normally.
5 years ago I would have said the majority of PFP patients I saw had weak quads causing PFP, but now I say the majority have PFP causing weak quads, and if we reduce PFP via other means we don’t increase the strength of the knee extensors, we DIS-inhibit them… we just allow them to work normally.
There are still some less common 1-in 50–100ish cases (in my clinical experience) that have a knee extension weakness causing PFP, interestingly these are often knee extension weakness secondary to other conditions that are lumbar spine or hip joint based.
Planes and Interventions
Another way to look the last 10–20 years of patellofemoral management is to visualise the interventions and how what forces they apply to the patella in terms of whether it is Sagittal Plane or Frontal Plane forces.
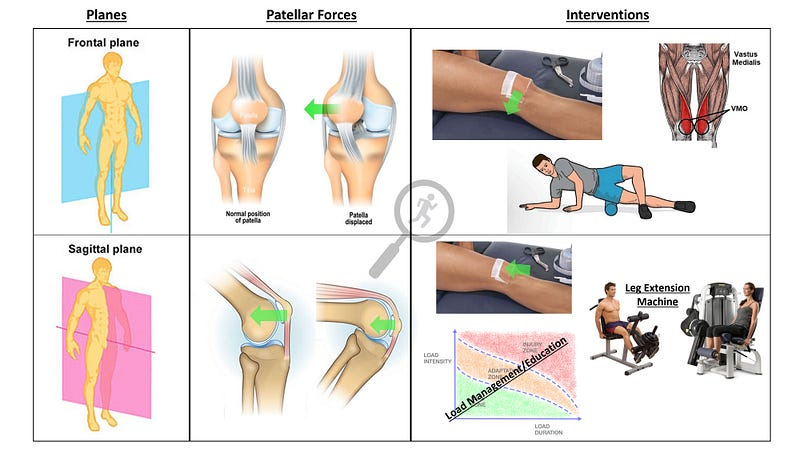
The bread and butter of the PFP management up until around 2010–2015 was focused on “patella tracking” and avoiding a lateral patellar force, best achieved by taping (direction doesn’t matter), VMO strengthening (can’t isolate it) and ITB rolling (to “lengthen it” — virtually impossible).
Since then the value of ‘sucking the kneecap into the groove’ with a sagital plane-compression force via quads ‘strengthening’/knee extension force production, and taping to hold the kneecap in the groove (sagital) rather than pulling it to the side (frontal) seems to have a higher value in keeping the kneecap joint happy.
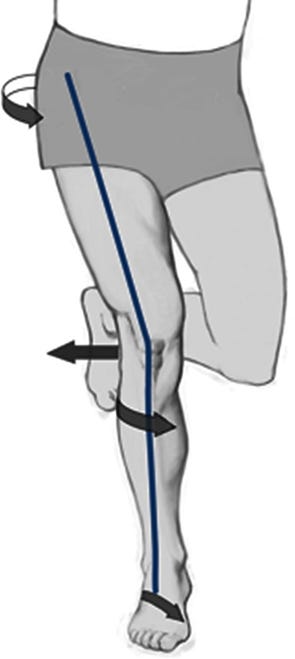
Another proposed contributer to ‘adverse’ sagittal front plane patellar forces is dynamic and forceful ‘Valgus’.
Gluteus Medius and the Battle against Valgus
Hip joint adduction and internal rotation movement during running, squatting and stair tasks is suggested to increase compressive loads at the PFJ, allegedly due to “poor gluteal function”.
However, this concept was founded from one study that focused on young female runners and the results weren’t that conclusive (Powers, 2010), further studies have shown only short-term effects only from targeting hip abductors/lateral rotators with ‘strength’ exercises (Fukuda et al., 2012) and recent reviews have even reported a lack of hip strength isn’t even predictive of developing PFP (Michael Skovdal Rathleff, Rathleff, Crossley, & Barton, 2014).
So does Hip Abductor weakness lead to pain? Or does pain lead to weakness (ie ‘Inhibition’) and hip muscle strength isn’t the magic bullet to target PFP (Thijs, Pattyn, Van Tiggelen, Rombaut, & Witvrouw, 2011).
To further debunk the “you only need to target posterolateral hip muscles for PFP reduction” concept a crafty and high quality study randomised 52 women with PFP into:
A posterolateral hip strength group (the traditional abductors and external rotators) and,
The other group did the complete opposite, anteromedial hip strength (adductors and internal rotators)
….and guess what?! They found that both groups showed improvement and there was no difference between the groups (Almeida, das Neves Rodrigues, Coelho, Rodrigues, & de Paula Lima, 2021).
So in summary, there is benefit to providing Hip Strength exercises for Patellofemoral pain and it doesn’t have to be specific.
The Consensus
The 2016 Patellofemoral pain consensus statement from the 4th International Patellofemoral Pain Research Retreat (Crossley et al., 2016) and more recently a living (…. on the living.. not the dead) systematic review with network meta-analysis (Winters et al., 2021) found that the most effective treatment for PFP is a combination of :
1. Education
2. Exercise (hip-based and knee-based)
3. Patellar Taping (Winters et al. included Patella Mobilisation here, Crossley et al. didn’t recommend it), and
4. Foot Orthoses (off the shelf).
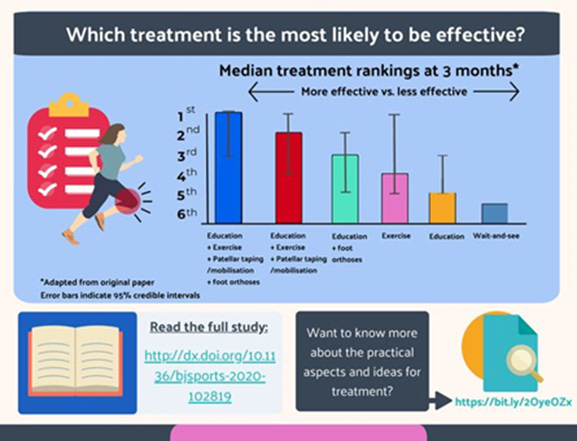
One big thing missing here in my opinion: education and activity modification, which in my experience has been crucial. Even though they mention ‘education’ I dug deeper into the Winters et al 2021 article in a previous blogpost and I found that their source for ‘education’.
The education was focused on the valgus knee-postures with activities, so presumably patients can continue doing everything with less valgus? In other words, ‘internal loads’ (postures, weaknesses, flexibility, joint tracking) are the focus and ‘external loads’ (activities, load) are lost in the noise”.
Even though the “education” in the above bar graph is low in effective management, sometimes education and activity modificaiton (dialling back up & downs) is all I do and they still get better.
My Thoughts
This is where the free preview ends. Paid subscribers now get access to the full post, including the clinical pearls, key takeaways, and practical recommendations.
Keep reading with a 7-day free trial
Subscribe to Nick Ilic | Physio Clinician to keep reading this post and get 7 days of free access to the full post archives.