

Clinician's Corner | Case Series: Good Sciatica Management is the Simple Stuff Done Well
A decade of stripping back to the evidence base. Two cases. Same outcome.
As this a longer article than usual I thought I’d introduce it and post a little video.
Yes, this is one of those blogs that you might get through over 2-3 sittings.
I thought about chopping it down into 2-3 separate posts but decided to go ahead with it and keep it all on one place.
This post has a free section and a paid section.
The free section covers what sciatica actually is and a short case study.
The paid section is the full documented case — start to finish — with MRI images, serial body charts, session notes, and the clinical commentary on what drove recovery.
If it’s useful, subscribing gets you the deeper case studies and longer pieces, and helps fund the time it takes to write them properly…. oh yes.. it also probably helps your patients.
This post is a guide only and not medical advice. It doesn’t replace assessment from a registered healthcare professional.
Sciatica is one of the most common things you’ll see in MSK practice.
It’s also, still, one of the most consistently mishandled. Patients arrive having been told to rest, handed a sheet of nerve stretches that wind them up, scanned before anyone’s laid a hand on them, and sent away without an explanation that makes sense of what’s happening in their leg. Nerves get pulled on when they’re already on fire. The metaphorical angry bear gets poked again and again. Recovery stalls. What should resolve in three months becomes twelve.
This isn’t a protocol piece. It’s a case series — two patients, documented start to finish, with serial body charts, session notes, MRI findings, and the actual language used at each stage.
The underlying premise running through it is simple:
Over a decade of stepping back to the evidence base — simplifying and stripping interventions back to what’s supported, being honest about what isn’t — hasn’t changed outcomes.
If anything, patients respond better when they understand why.
Call it “better bang for the buck”, or call it “Integrity meeting simplicity in the management of something complex”. What you end up running is essentially a triage, safety-net, and coaching service - but with qualified expertise lying underneath for those small adjustments or red flag spotting and signposting.
Patients understand the plan, consent to it genuinely, and appreciate the honesty far more than they'd appreciate another passive treatment that temporarily shifts a number on a pain scale.
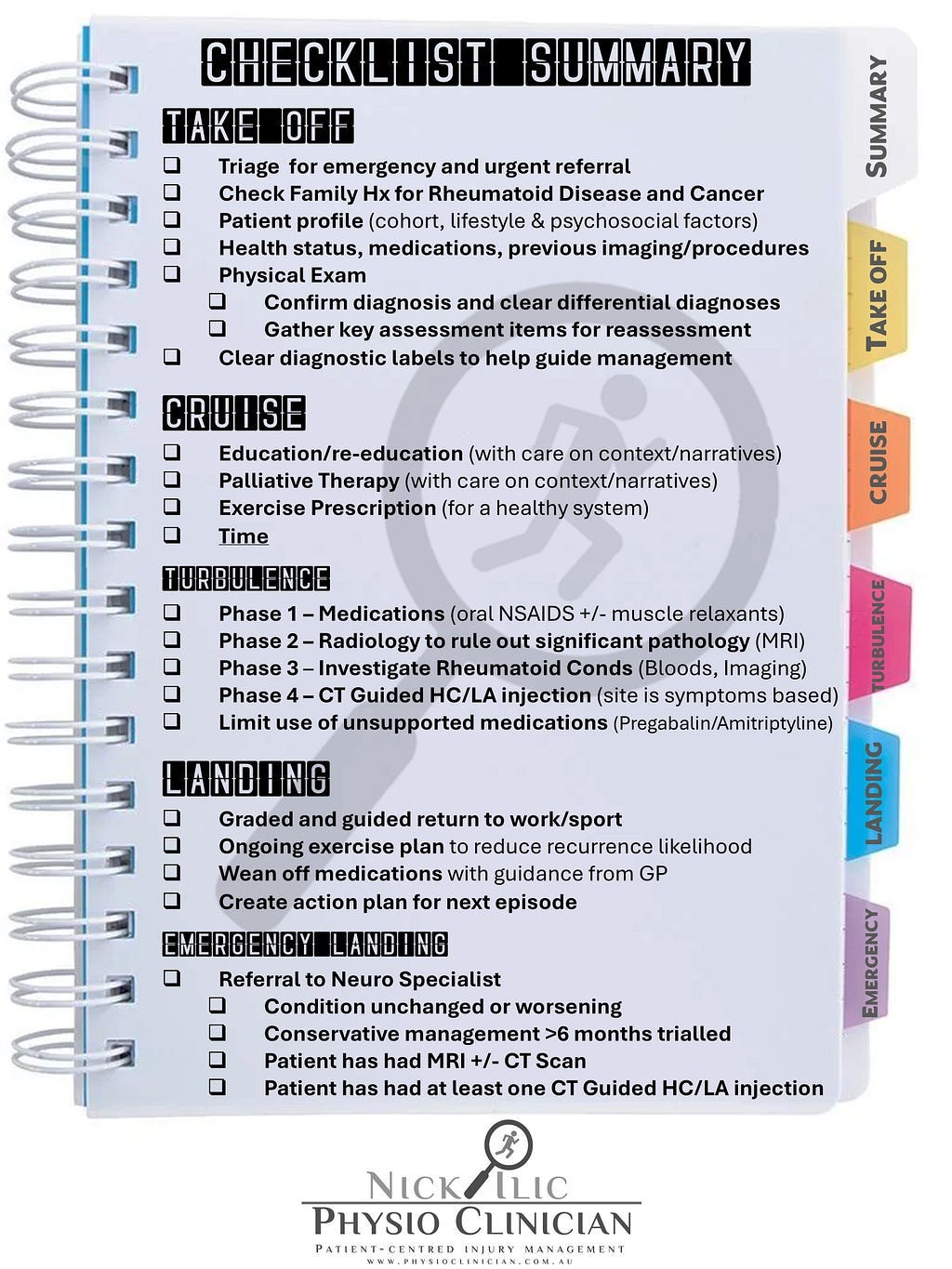
This piece sits alongside the back pain checklist published earlier in this series — Take-off to Touchdown: A Pilot’s Checklist — which covers the broader assessment and management framework.
That’s the structure; this is what it looks like applied to a real diagnosis over five months.
Here’s todays menu:
Both patients in this case series consented to anonymous sharing of their cases, including imaging.
What sciatica actually is — and what it isn’t
The word sciatica has outlived its clinical usefulness.
It’s an archaic, imprecise label applied to leg pain of wildly varying origin, mechanism, and prognosis — which is exactly why it leads to misdiagnosis and, sometimes, inappropriate surgery [1, 2].
Population Sciatica prevalence sits around 3–5%, with peak incidence in the 40s for men and 50s for women, as part of the normal degenerative spinal process [1].
None of that is surprising.
What matters clinically is getting the terminology right from the outset, because what you call it shapes how you manage it and what you tell the patient.
For example: "Glute tightness" or "Piriformis Syndrome" is not useful (unless of course, as a Clinician, you’re a one-trick pony with massage, stretches and dry-needling as your hammer, and tightness as your nail.)
It doesn't get the patient any closer to understanding what's actually happening in their leg, and it sends management down a path that may actively make things worse.

Radicular Pain vs Radiculopathy - Gain vs Loss
I’ve stopped worrying about using the word “radicular” with patients. They’re adults — big boy, big girl pants. They can handle the terminology, and I’d argue it serves them better than “sciatica” ever did.
Especially once you explain where it comes from. Rādīcula — Latin for “little root.” The nerve root.
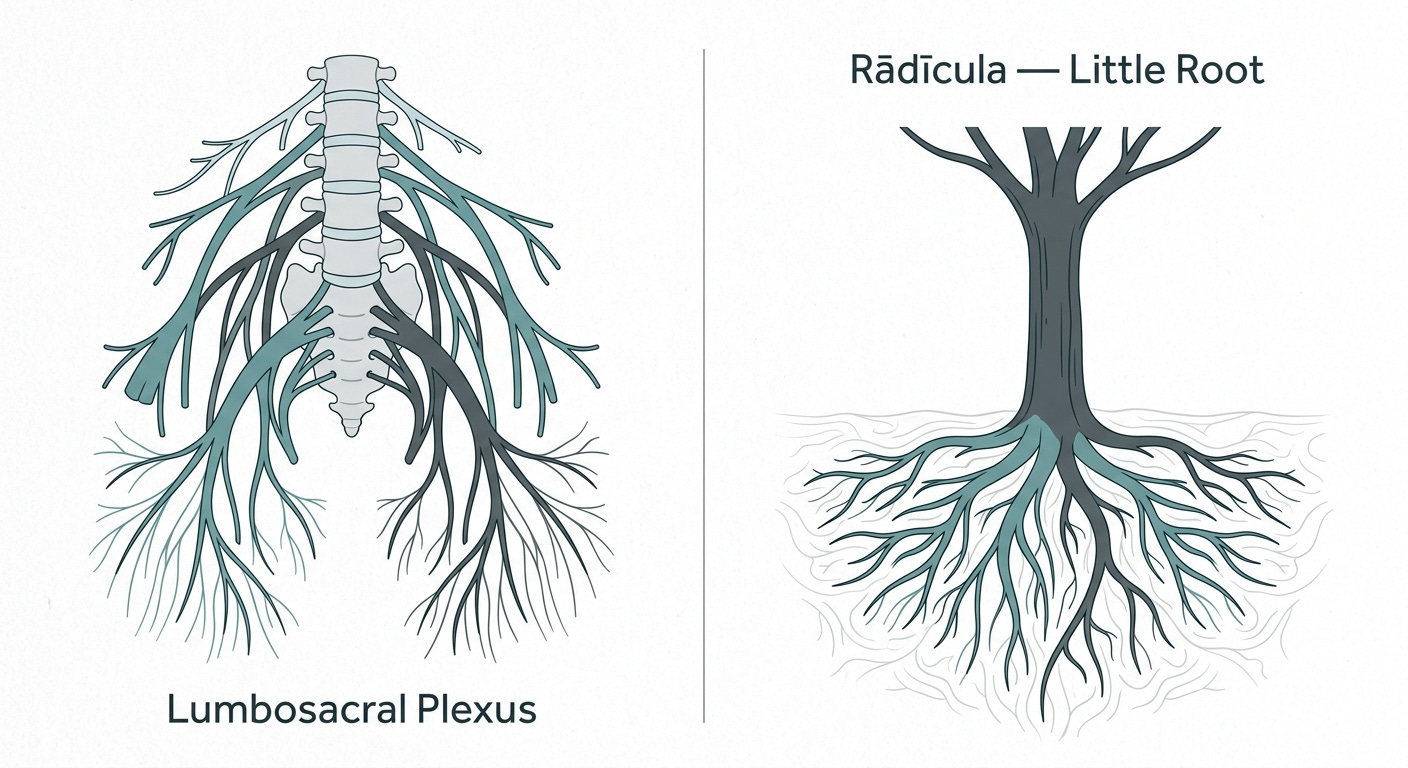
Suddenly it’s not a scary medical word, it’s a description. You’re telling them their root hurts. Most patients find that more meaningful, less threatening, and easier to remember than a vague anatomical eponym that’s been applied to everything from a slipped disc to a tight piriformis.
I covered the full differential between radicular pain, radiculopathy, and somatic referred pain in an earlier piece — Let’s talk about ‘Armatica’ — worth reading alongside this if you want the complete picture.
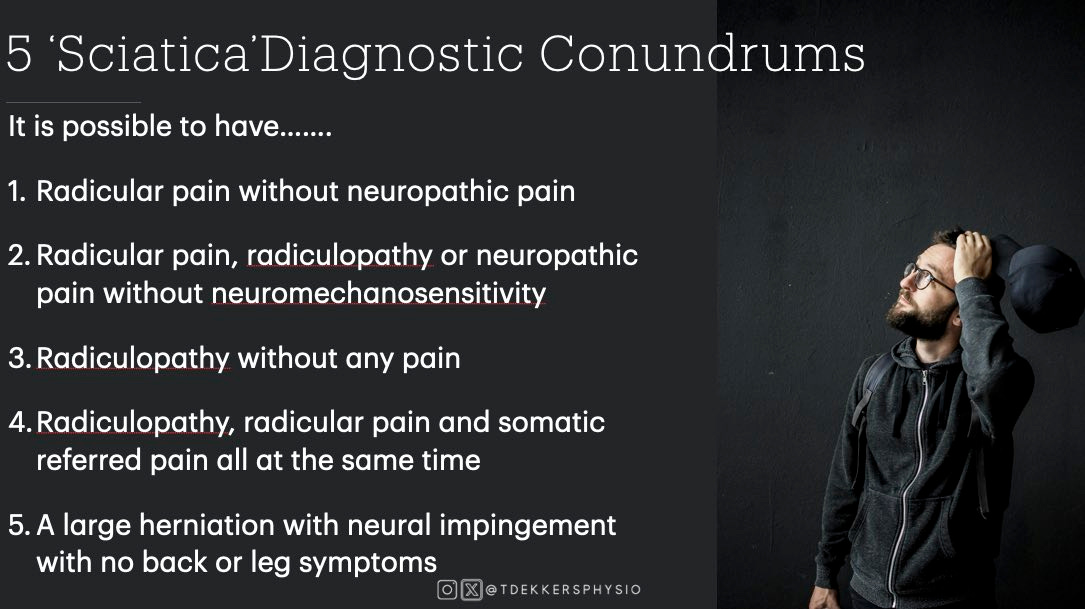
The first distinction worth being precise about: radicular pain is not the same as radiculopathy [2, 3].
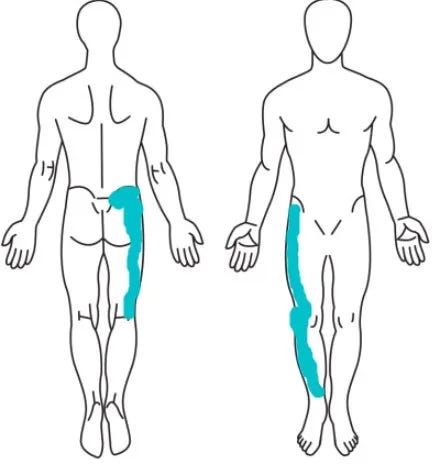
Radicular pain is ... pain. But doesn't include changes in sensory or motor function. In the lumbar spine radicular pain is most often sharp, lancinating, electric-shock-like pain travelling down the limb in a narrow band [3]. Sometimes it's achy, but the lancinating quality is the classic. Interestingly, cervical radicular pain tends to present more as ache than as the textbook electric shock — worth keeping in mind when you're applying the same language across regions.
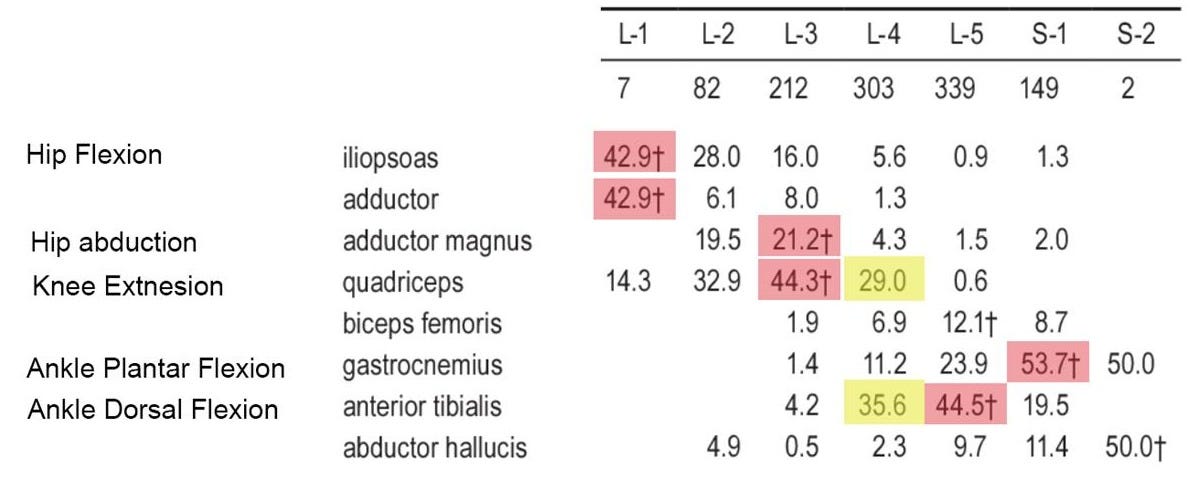
Radiculopathy is a loss of sensory or motor function — a conduction block along a spinal nerve, but it does not include pain. Radiculopathy is identified by sensory loss in a dermatomal distribution, myotomal motor weakness, or diminished deep tendon reflexes [3, 4]. Loss of L5 dorsiflexion strength. Loss of S1 Achilles reflex. Loss of L3 quadriceps power. Not complete loss — there’s significant overlap between nerve fibres — but a measurable decrement.
I thought I once heard a ‘Radicular Wizard’ (RW) once say: “Radiculopathy is a CHANGE in sensory or motor function” (rather than loss), as sometimes there can be hyperreflexia on tendon reflex testing. But I recently poked Grand RW Tom Jesson on this point and he assures me: “No Nick… it’s a loss. You’re on the magic mushrooms again.”
Radicular Pain and Radiculopathy often coexist, but not always. A patient can have severe radicular pain with no objective deficit. A patient can have significant motor loss with minimal pain. ‘Cycling Simon’, in this case series, is a textbook example of the latter — he didn't even know what his problem was, he just thought he was "walking different."
Sciatica is less common than you’d think
Cycle through a week of new patients with leg or lower back symptoms and the truly nerve-root-related cases account for only around 8–10% of presentations [2]. Far more common is non-radicular low back pain — discogenic pain, facet joint pain, sacroiliitis, upper lumbosacral pain, or the broad bucket of nonspecific low back pain where pinning down a specific diagnosis doesn’t actually change management.
The reason radicular pain is worth diagnosing accurately — even when non-specific low back pain mostly isn’t — is because the prognosis is genuinely different, and the management changes accordingly. Lumping radicular pain in with nonspecific LBP and telling the patient “six to twelve weeks” undersells the timeline, creates false expectations, and erodes trust when recovery takes longer.
What else can cause leg symptoms
The differential for “leg pain that looks radicular” is broader than the lumbar spine.
Peripheral neuropathy can occur anywhere along the sciatic nerve tree from buttock to foot.
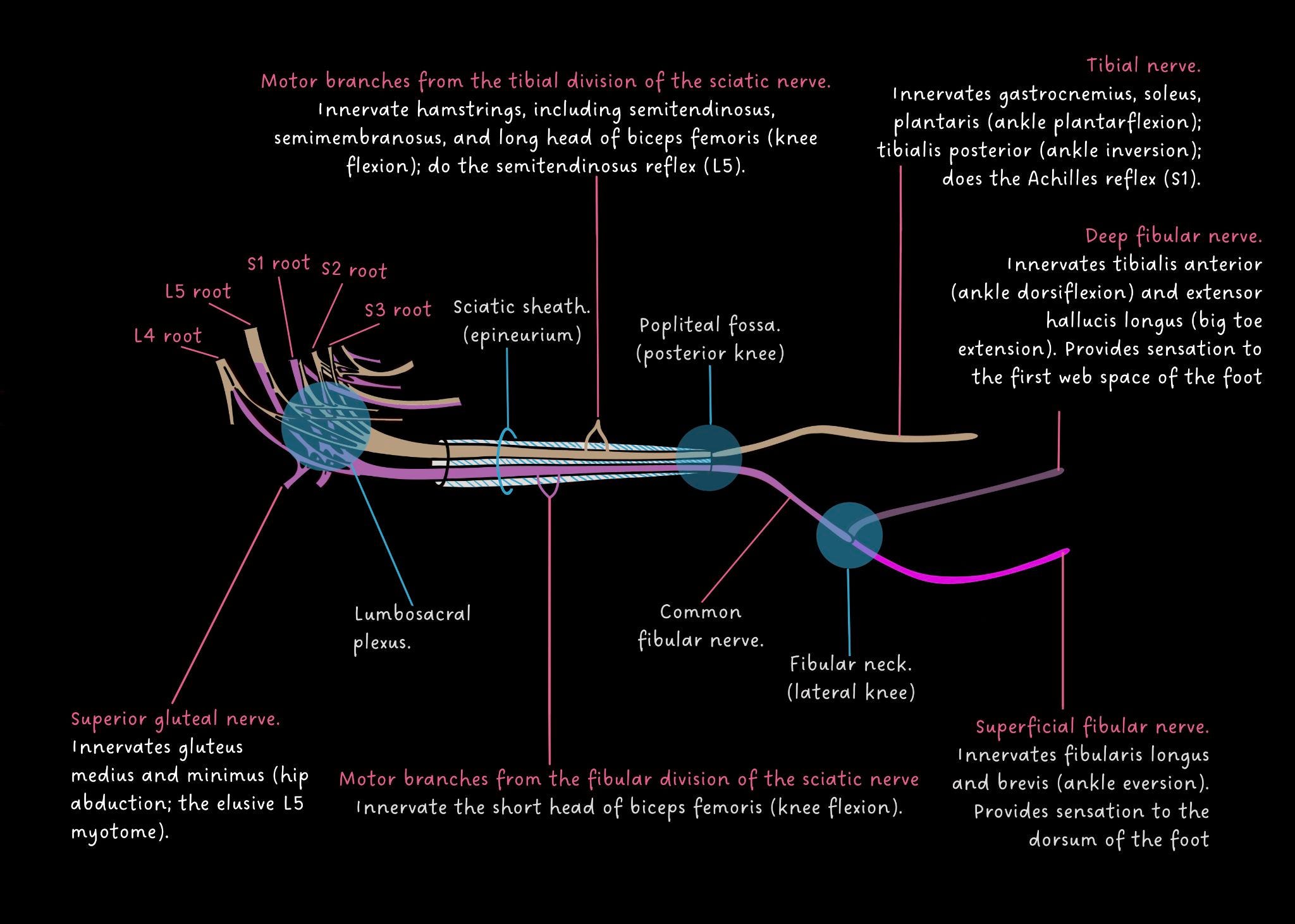
Hip joint, SIJ, and visceral structures can all refer pain into the lower limb — a topic covered in depth in the Hip Joint, SIJ and Lumbar Spine differentiating post. It’s our job to safety-net and screen these things — not just stamp a sciatica label on every patient with leg pain.

And, frankly, we’re better placed than a primary care GP to do this work, because we have the assessment time and we have the gear — dynamometry to objectively measure strength loss in radiculopathy, for example.
Worth flagging too: bilateral diffuse leg symptoms that don’t fit the usual buckets should prompt a medication review - not just Cauda Equina Syndrome follow up questions. Statin myopathy is an under-recognised confound that can present convincingly as a mechanical lower limb problem.
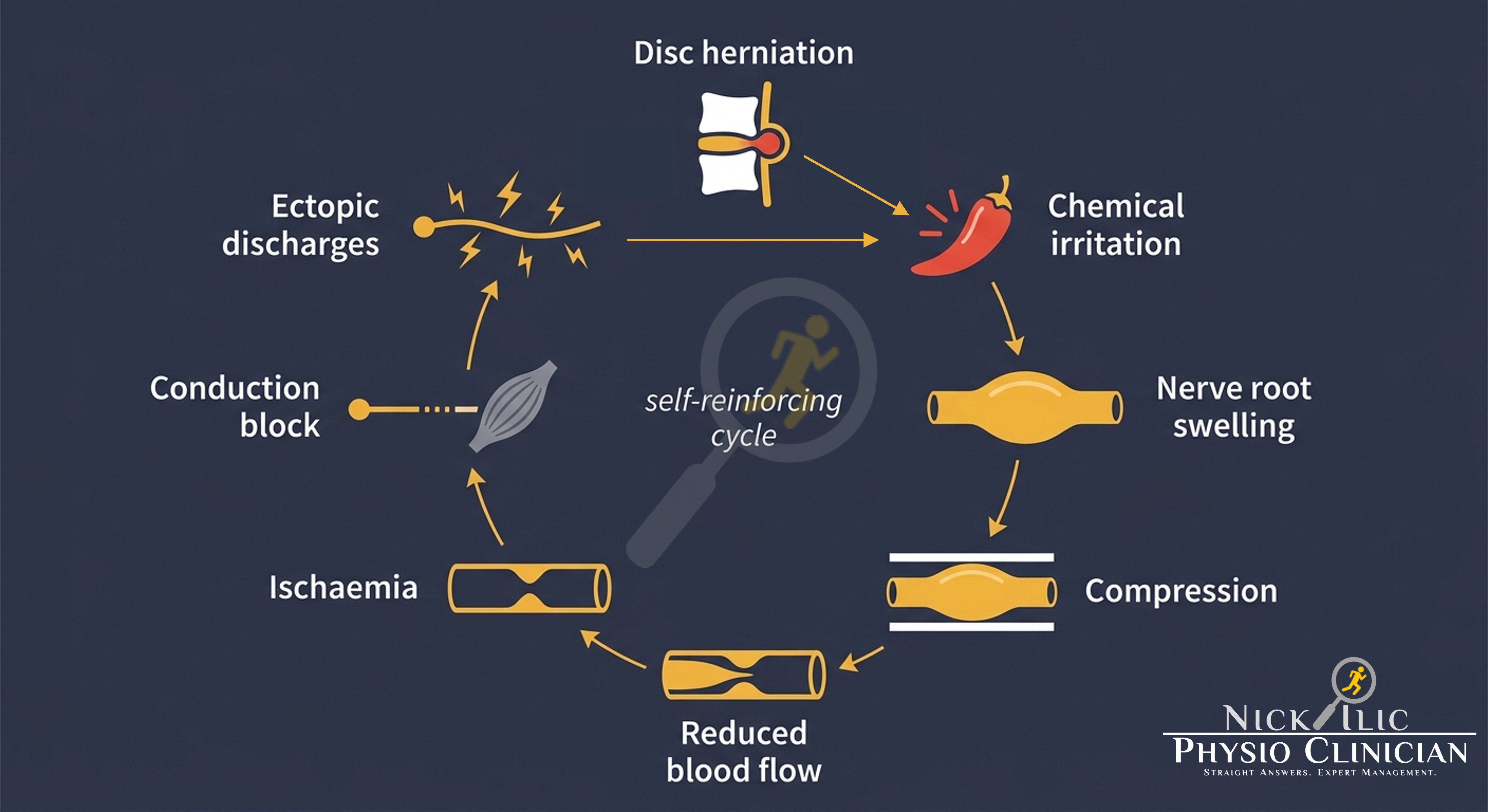
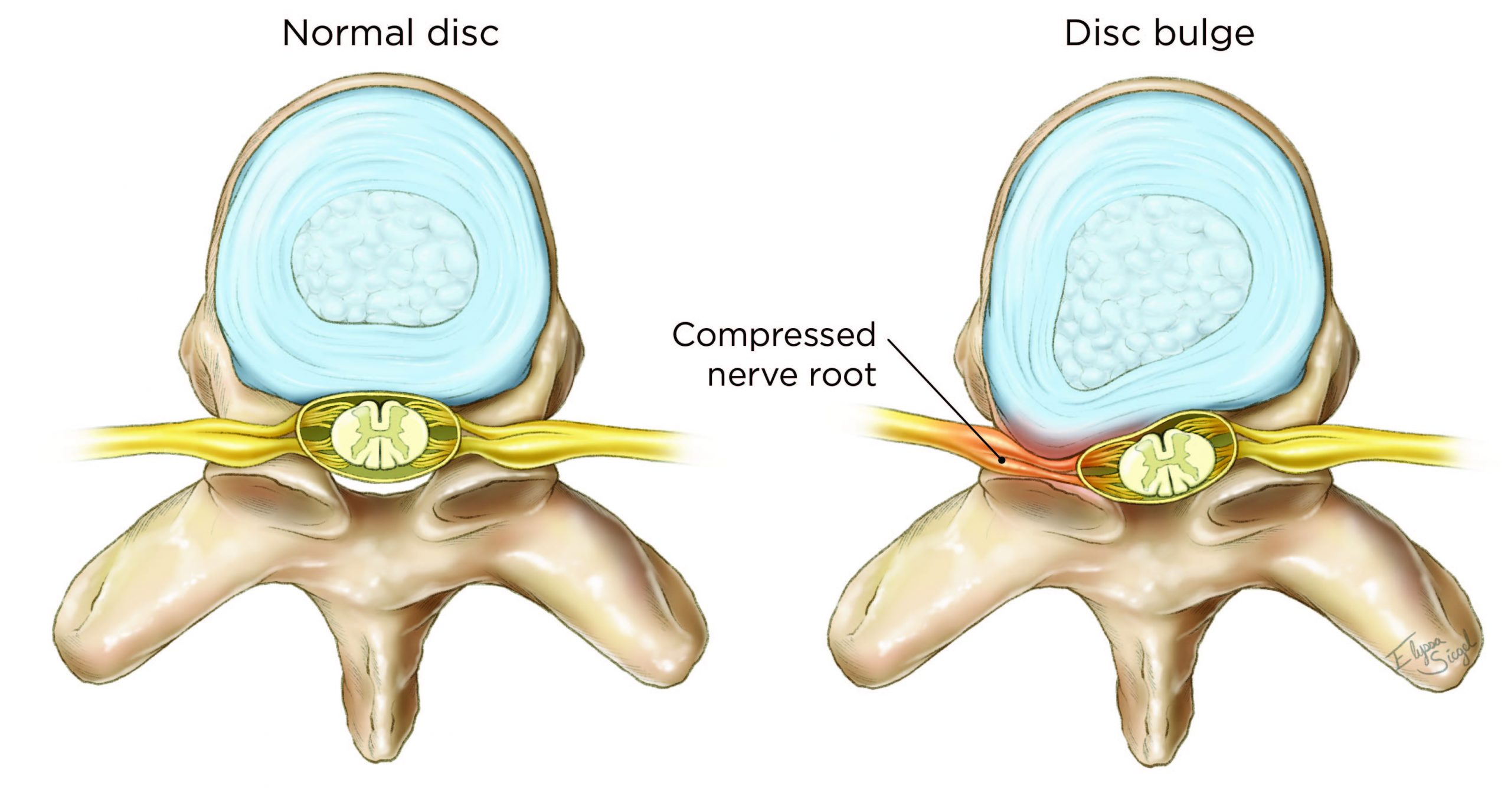
The compression negative feedback cycle
Disc bulge / herniation can lead to:
Chemical irritation + inflammation → Nerve root swelling → Less space / more compression → Reduced blood flow → Ischaemia → Conduction block = weakness / numbness → Ectopic discharges = sciatica pain → More irritation / more swelling → Repeat loop
The compression-symptoms disconnect
Here’s the thing about nerve root pain — compression alone usually isn’t the problem. Healthy nerve roots are actually fairly tolerant of being nudged. What they’re not tolerant of is being nudged while on fire.
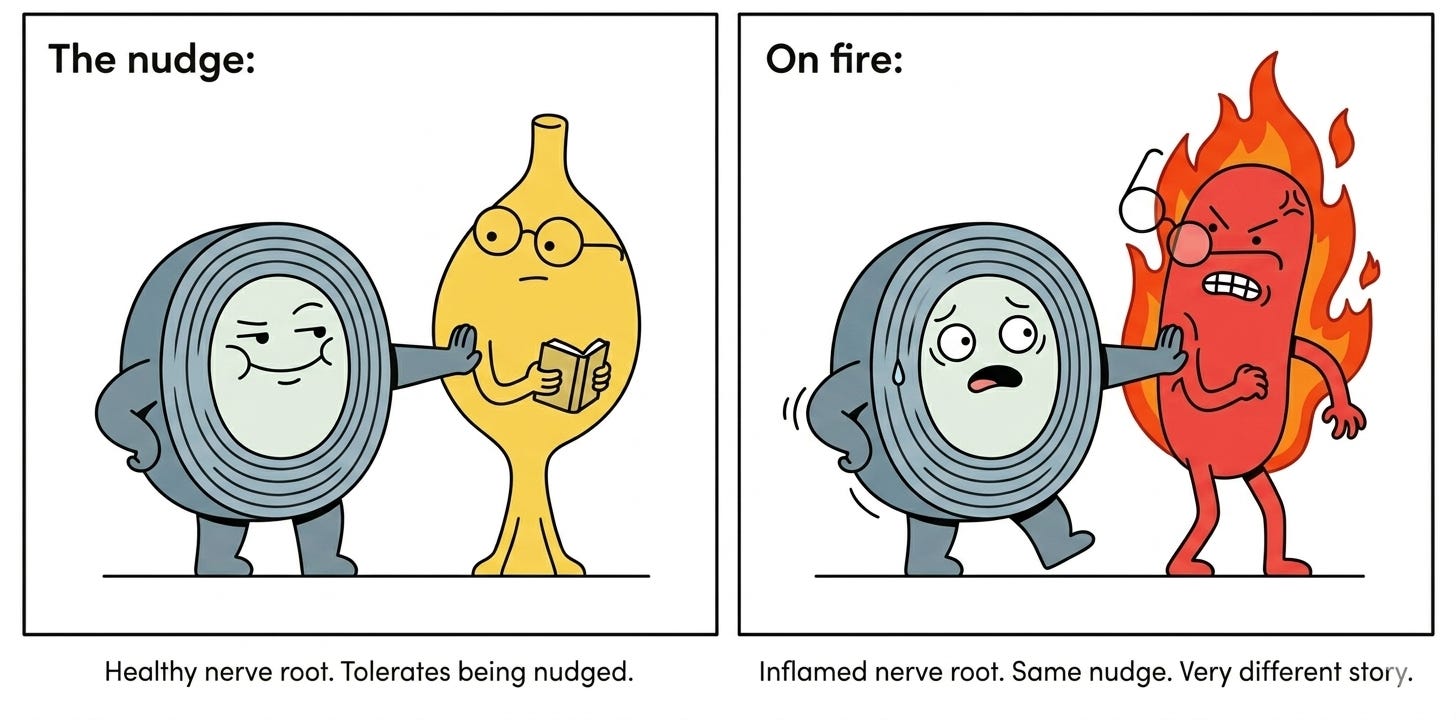
When disc material contacts the nerve root, the body mounts an immune response — TNF, phospholipase A2, the whole inflammatory toolkit — and the nerve root ends up sitting in a chemical bath, swelling in a space that has nowhere to go [2, 5]. A miniature compartment syndrome, essentially.

Size of the herniation? Largely irrelevant to how much it hurts. A small protrusion in a high-inflammation environment can be far more symptomatic than a large one that isn’t [2].
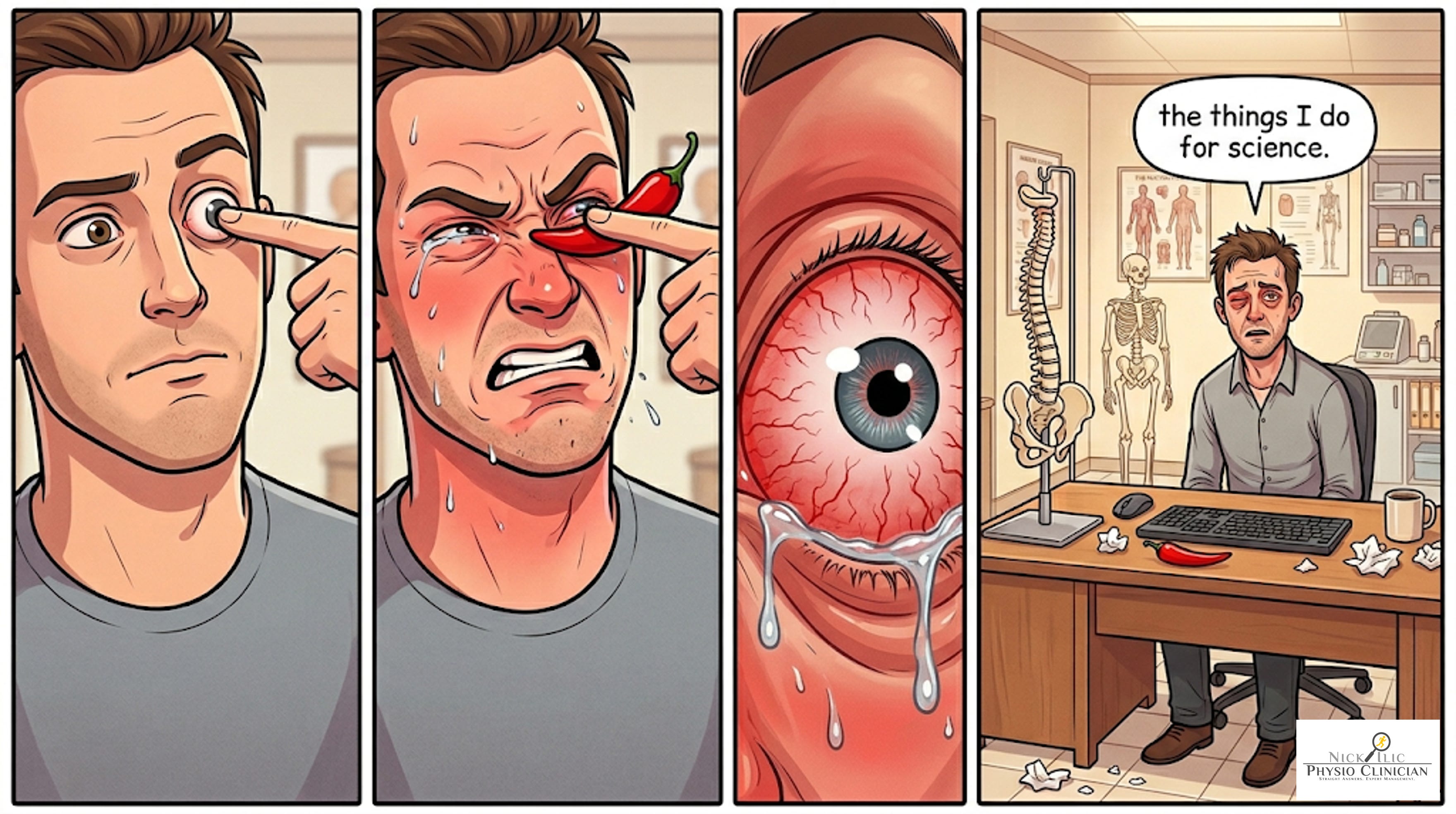
Tom Jesson’s analogy lands well in clinic: think of the disc as a finger pressing on the eyeball [2].
On its own, uncomfortable but manageable. But poke the eyeball with chilli powder on the finger, and even a light touch becomes agonising.
That’s the inflamed nerve root. The chilli is the inflammation.
It’s not about how hard the finger presses — it’s about what’s on it.
This framing works both ways. It explains why an inflamed nerve root hurts so much even with a relatively small structural change. And it also lets you defuse incidental imaging findings — if testing suggests no radicular involvement and the patient has been told their MRI shows a "bulging disc," you can use the same analogy in reverse: the finger might be there, but without the chilli powder it doesn't have to mean anything.
This disconnect is confirmed by asymptomatic population imaging:
Disc protrusions are found in 29% of 20-year-olds and up to 43% of 80-year-olds with no pain [2].
22% of asymptomatic subjects show nerve root compression on imaging [2].
Radicular pain is a clinical diagnosis. The scan confirms and contextualises. It doesn’t lead.
See also: Schmorl’s Nodes are Puzzling — another good example of imaging findings that look alarming and mostly aren’t.

{kind=link}
Case 1 — Cycling Simon
Suspected right L5/S1 foraminal impingement · Traumatic onset · Resolved 6–8 weeks post-injury
This case is brief — partly by design, partly because the patient himself made it easy. Simon came in for the initial assessment and a single follow-up. The rest was managed by email.
At around 30-40km/hr, he had to suddenly stabilise himself and stick his right leg out from the pedal and his right foot struck the ground with a semi-decent jarring force. Fortunately, the leg was extended in a way that he was able to attenuate that force from the ankle right up into his hip and lower back.

At the time, symptoms were ankle-localised. Over the following weekend, a mixed lumbosacral/radicular pattern emerged: right upper buttock spreading posterolaterally to the knee, then distally to the anterior shin.
The first visit was diagnostically ambiguous.
Pain was constant at presentation. Simon was visibly antalgic, with a significant weight shift to the left during squat that he hadn’t noticed until it was pointed out.
Lumbar spine clear on ROM testing.
Hip testing mildly positive bilaterally on full Flexoin + FADIR.
R ASLR was mildly painful - SIJ compression offered some symptom relief.
Other SIJ cluster tests unremarkable.
He had a 10-20% weight shift to the unaffected side during gait.
Do you know how some patients are in pain, some others are in suffering? Simon was just in pain, it wasn’t phasing him too much, just annoying.
My impression at that stage: A mixed presentation of hip/lumbosacral pain from having the leg jammed up in to the hip with moderate force. But not enough force to cause any significant long-term injuries, just an awkward force. A very linear force too, basically femur shoved into pelvis, pelvis shoved into lumbar spine.
Given the lumbar spine looked good on assessment (when it shouldn’t have if it was an issue), and the hip/SIJ on the affected side were equally irritable (mild-moderate) and he was otherwise fine and dandy, other than taking oral NSAIDs for 4 days or so we decided to: get on with life and track it.
Cycling Simon is the Mall Cop of this case series.
Observe. Report. Let the body do its job.
")
No treatment, just assessment, reassurance, education, load modification and wait and see.
Follow-up — motor deficit confirmed
At the two-week follow-up, pain had completely settled.
He was going to cancel that appointment, but Simon reported a gait pattern he couldn’t account for: unable to heel walk and restricted ankle range of motion – as such he was “walking funny”.
He was completely clear on regional assessment, lumbosacral, hip, knee, ankle, even pinky toe.
But, his gait looked like this - watch that right foot:
Yep - ‘Tipsy Pirate Syndrome’.
In swing phase there was a slight swinging/circumduction of the right leg around the side. Suspecting a dorsiflexion issue from his subjective, I asked him to walk on his heels, toes in the sky.
Who doesn’t love a 1990s crime show dramatic re-enactment…. might as well keep that going - with some added assistance from our Clinical K9 unit.
Yep.. you guessed it, dorsi flexion lacking.
Out came the handheld dynamometer. In my case, the AXiT Push-IT.
Right ankle dorsiflexion force production was reduced by approximately 44% (11.3kg vs 20.30kg).
The presentation had shifted from pain-dominant to motor deficit-dominant. A pain-free radiculopathy.
Given the mechanism and recent of the injury, and the relatively quick resolution of pain (3-4 weeks), I had a strong suspicion that this short-term radiculopathy would resolve with time and the patient could continue is regular activities, but not running until strength returned.
Management of Tipsy Pirate Syndrome*
*not a real syndrome
Education was provided on the expected mechanism, foraminal impingement of the right L5 spinal nerve root: “the window closed suddenly and compressed the nerve going through it and the nerve is probably a little swollen and irritable but should settle down.”
An emailed program explaining this was provided to him for him to refer back to. The door was left open for him to come back in at any time.
His response to email follow-up 2 weeks later:
“Fortunately I’m better than I’d hoped, my strength has returned and I’m back to everything”…
Full resolution was around 6-8 weeks. Minimal intervention, just wait and see.
But that was a weird short-term case in a patient well known to me who just wanted to check and make sure things were ok…. Many of those sorts of cases resolve without patients seeking assessment or treatment.
For a full blown Sciatica Case, acute disc herniation, radicular pain and radiculopathy– that’s not usually the case, so let’s meet Deadlift Derek.
